Sa?l?k ?al??anlar?nda t?berk?lin cilt testi ile QuantiFERON-TB Gold-In Tube testinin kar??la?t?r?lmas?
Vildan
?A?LAYAN1, ?znur AK2, G?l DABAK3, Ebru
DAMADO?LU4, Banu KETENC?5, M?ge ?ZDEM?R3,
Serdar ?ZER2, Attila SAYGI3
1 SB Tekirda? G???s Hastal?klar? Hastanesi, Tekirda?,
2 SB Kartal L?tfi K?rdar E?itim ve Ara?t?rma Hastanesi, ?nfeksiyon Hastal?klar? ve Klinik Mikrobiyoloji Klini?i,
?stanbul,
3 SB S?reyyapa?a G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi, ?stanbul,
4 Hacettepe ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Eri?kin Allerji ?nitesi, Ankara,
5 Dr. Siyami Ersek G???s, Kalp ve Damar Cerrahisi E?itim ve Ara?t?rma Hastanesi, G???s Hastal?klar? Klini?i,
?stanbul.
?ZET
Sa?l?k ?al??anlar?nda t?berk?lin cilt testi ile QuantiFERON-TB Gold-In Tube testinin kar??la?t?r?lmas?
Prospektif, kesitsel ve g?zlemsel nitelikteki ?al??mam?z?n amac? sa?l?k ?al??anlar?nda latent t?berk?loz infeksiyonu tan?s?nda, t?berk?lin cilt testi (TCT) ile QuantiFERON-TB Gold-In Tube (QTF-GIT) testini kar??la?t?rmakt?r. ?al??ma, ayn? ???nc? basamak g???s hastal?klar? ve t?berk?loz e?itim hastanesinde ?al??an 78 g?n?ll? sa?l?k ?al??an?n? i?ermektedir. Aktif t?berk?lozu, imm?nyetmezli?i ya da maln?trisyonu olanlar ?al??maya dahil edilmemi?tir. TCT Mantoux metoduyla uyguland?. ESAT-6, CFP-10 ve TB7-7 antijenleri kanda interferon-gama (IFN-γ) ara?t?r?lmas? i?in kullan?ld? (QTF-GIT). BCG skar say?s? ile TCT end?rasyon ?ap? aras?nda istatistiksel olarak anlaml? ili?ki saptand? (p< 0.01). QTF sonu?lar? ve ?nceki BCG a??lamas? aras?nda anlaml? bir ili?ki yoktu (p> 0.05). ?ki test aras?nda orta d?zeyde uyum mevcuttu (κ: 0.346). QTF-GIT testinin duyarl?l??? %56.14 (TCT ve QTF-GIT pozitif), ?zg?ll??? %90.48 (TCT ve QTF-GIT negatif), pozitif kestirim de?eri %94.12, negatif kestirim de?eri %43.18, do?ruluk oran? da %65.38 olarak saptand?. QTF sonucuyla TCT end?rasyon ?ap? aras?nda anlaml? d?zeyde ili?ki mevcuttu (p< 0.01). QTF-GIT testine g?re ?al??ma pop?lasyonumuzdaki latent t?berk?loz infeksiyon prevalans? %43, TCT'ye g?re %73 idi ve BCG a??lanma oran? %87 idi. Sonu? olarak; TCT ?nceki BCG a??lanmas?ndan etkilenmi?, buna kar??n QTF-GIT etkilenmemi?tir. Rutin BCG a??lama program? olan toplumlara latent t?berk?loz infeksiyonu tan?s?nda TCT'ye alternatif olarak QTF-GIT testini ?nerebiliriz.
Anahtar Kelimeler: T?berk?lin cilt testi, QuantiFERON-TB Gold-In Tube, latent t?berk?loz infeksiyonu, t?berk?loz.
SUMMARY
Comparison of tuberculin skin testing and QuantiFERON-TB Gold-In Tube test in health care workers
Vildan
?A?LAYAN1, ?znur AK2, G?l DABAK3, Ebru
DAMADO?LU4, Banu KETENC?5, M?ge ?ZDEM?R3,
Serdar ?ZER2, Attila SAYGI3
1 Tekirdag Chest Diseases Hospital, Tekirdag, Turkey,
2 Department of Infectious Diseases and Clinical Microbiology, Kartal Lutfi Kirdar Training and
Research Hospital, Istanbul, Turkey,
3 Sureyyapasa Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey,
4 Adult Allergy Unit, Department of Chest Diseases, Faculty of Medicine, Hacettepe University,
Ankara, Turkey,
5 Department of Chest Diseases, Dr. Siyami Ersek Chest and Cardiovascular Surgery Training and
Research Hospital, Istanbul, Turkey.
The purpose of this prospective, cross-sectional observational study was to compare the tuberculin skin testing (TST) with QuantiFERON-TB Gold-In Tube (QTF-GIT) for the detection of latent tuberculosis infection in healthcare workers (HCWs). The study included 78 volunteers who are HCWs at the same tertiary care teaching hospital for chest diseases and tuberculosis. Participants with active tuberculosis, immunodefficiency or malnutrition were not included. The TST was administered by the Mantoux method. Peptides representing ESAT-6, CFP-10 and TB7-7 were used as TB-specific antigens in the whole-blood Interferon-gamma (IFN-γ) assay (QTF-GIT). There was a statistically significant relation between the number of Bacillus Calmette-Guerin (BCG) scars and the diameter of TST (p< 0.01). QTF results according to previous BCG vaccinations did not significantly differ (p> 0.05). There was an intermediate concordance between two tests (k: 0.346). QTF-GIT has a sensitivity of 56.14% (both TST and QTF-GIT are positive), specificity of 90.48% (both TST and QTF-GIT are negative); positive predictive value of 94.12% and negative predictive value of 43.18% and accuracy is 65.38%. There was a statistically significant relation between TST diameter and QTF result (p< 0.01). Latent tuberculosis infection prevalance of our study population was 43% according to QTF-GIT test, 73% according to TST and BCG vaccination rate was 87%. In conclusion, TST is affected by previous BCG vaccinations, QTF-GIT is not. We can recommend QTF-GIT test for the detection of latent tuberculosis infection as an alternative to TST in populations with routine BCG vaccination programme.
Key Words: Tuberculin skin testing, QuantiFERON-TB Gold-in Tube, latent tuberculosis infection, tuberculosis.
Tuberculosis (TB) infects an estimated one third of the world's population, and about 9 million cases occur every year (1,2). Because infected individuals eventually present to health care providers, health care workers (HCWs) are especially vulnerable to TB exposure and infection (3). All health care workers who have duties that involve face-to-face contact with patients with suspected or confirmed TB disease (including transport staff) should be included in a TB screening program (4).
Until recently, skin testing with purified protein derivative (PPD) of tuberculin was the only practical way of detecting latent Mycobacterium tuberculosis infections (5). The main drawback of the tuberculin skin test (TST) is poor specificity due to previous vaccination with Bacille Calmette-Guerin (BCG) and exposure to nontuberculous mycobacteria (NTM). Therefore, this test overestimates the population at risk (5,6). Interferon-gamma (IFN-γ)-Release Assays (IGRA) have been developed as a potential replacement for the TST. QuantiFERON?-TB Gold-In Tube (QTF-GIT) is a whole blood IGRA and uses a mixture of two antigens that are encoded by the Region of Difference 1 (RD1) to stimulate T lymphocytes. These antigens are the Early-Secreted-Antigenic-Target 6 (ESAT-6) and Culture-Filtrate-Protein-10 (CFP-10); in addition, the mixture contains TB7-7, a third, M. tuberculosis-specific antigen (1,6). The advantages of these new assays over the TST are the higher specifities (excluding false-positive results due to BCG or environmental mycobacteria), logistic simplicity, and need of only one patient visit (5,6,7).
The purpose of this prospective, cross-sectional observational study was to compare the TST with QTF-GIT for the detection of latent tuberculosis infection in healthcare workers.
MATERIALS and METHODS
The present study was conducted at Heybeliada Chest Diseases and Chest Surgery Training and Investigation Hospital during the year 2005. It is a tertiary care teaching hospital for chest diseases and tuberculosis. The study included 78 volunteers who are HCWs at the same hospital. HCWs who have active tuberculosis, immunodefficiency or malnutrition were not included.
Age, gender, occupation, the duration of work, any accompanying diseases that can be a risk factor for tuberculosis, past tuberculosis history, tuberculosis contact history outside the hospital and previous TST results were recorded in a questionnaire. The number of previous BCG vaccinations were also recorded. All volunteers had a new postero-anterior chest X-ray.
The TST was administered by the Mantoux method using 0.1 mL (5 TU) of Tubersol. Transverse induration at the TST site was measured by the same trained healthcare worker after 72 hours according to "T.C. Sa?l?k Bakanl??? Verem Sava?? Daire Ba?kanl???" recommendations. Indurations of 15 mm and more in BCG vaccinated, and 10 mm and more in unvaccinated HCWs were considered positive. Repeat TST was performed to TST negative cases after a week due to booster phenomenon, and the second TST was evaluated.
Pool of overlapping peptides representing ESAT-6, CFP-10 and TB7-7 were used as TB-specific antigens in the whole-blood IFN-γ assay. The test and the interpretation results were performed according to the manufacturer's instructions (Cellestis Ltd, Carnegie, Victoria, Australia).
RESULTS
The study was conducted at Heybeliada Chest Diseases and Chest Surgery Training and Investigation Hospital between 01-31 August 2005. Thirty-three women (42.3%) and 45 men (57.7%) with a total of 78 HCW were included in the study. Mean age of the study population was 30.51 ? 8.57. Table 1 shows the distribution of patients with respect to job category.

There was a statistically significant relation between the number of BCG scars and the diameter of TST (p< 0.01). The diameter of TST was significantly higher in HCWs with two BCG scars than HCWs with one scar (p= 0.002; p< 0.05) and HCWs without a BCG scar (p= 0.03; p< 0.05). The diameter of TST was significantly higher in HCWs with three BCG scars than HCWs with one scar (p= 0.04; p< 0.05). Table 2 shows the TST results with respect to BCG scar number.

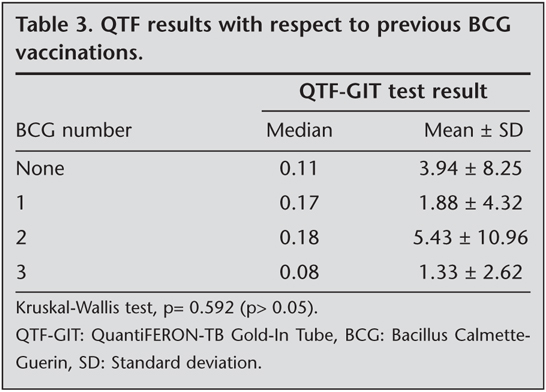
QTF results according to previous BCG vaccinations did not significantly differ (p> 0.05). Table 3 shows the QTF results with respect to previous BCG vaccinations. Concordance between test results from the TST and QTF-GIT assay was assessed using k coefficient (k: 0.346) and there was an intermediate concordance between two tests. QTF-GIT has a sensitivity of 56.14% (both TST and QTF-GIT are positive), specificity of 90.48% (both TST and QTF-GIT are negative); positive predictive value of 94.12% and negative predictive value of 43.18% and accuracy is 65.38%. Table 4 shows the correlation between QTF-GIT and TST.

While QTF was positive in 91.2% of cases when TST was 10 mm or more, it was positive in only 2.9% of cases with TST diameter of 0 mm. There was no QTF positive case when TST diameter was between 5-9 mm. There was a statistically significant relation between TST diameter and QTF result (p< 0.01). Table 5 shows the correlation of TST diameter and QTF result.

There was not a statistically significant relation between TST results and years served in the health care profession (p> 0.05). However, there was a statistically significant relation between the years served in the health care profession and QTF result (p< 0.05). Table 6 shows the effect of years served in the health care profession to TST and QTF results.

Latent tuberculosis infection prevalance of our study population was 43% according to QTF-GIT test, 73% according to TST and BCG vaccination rate was 87%.
DISCUSSION
In many developed countries (e.g., United States and Canada), HCWs are screened with TST to identify and treat latent TB infection (3,8). However, effective screening requires a test that can accurately and reliably diagnose latent tuberculosis infection and predict those most likely progress to disease (9). QTF overcomes some of the shortcomings of the TST, namely, the need for return visits, reader variability, variable specificity, cross reactivity with BCG vaccine and non-tuberculous mycobacterial infection (10,11). The QuantiFERON-TB Gold test (Cellestis Ltd, Carnegie, Victoria, Australia), which is based on a whole-blood ELISA developed in the late 1980s, has been recently approved for in vitro diagnostics by the U.S. Food and Drug Administration, and a guideline from the U.S. Centers for Disease Control and Prevention has been published (12). In-tube test is a newer version of the QuantiFERON-TB Gold assay. In the present study, we evaluated the QTF-TB Gold in Tube Test (Cellestis Ltd, Carnegie, Victoria, Australia) and TST results of health care workers in a tertiary care teaching hospital for chest diseases and tuberculosis.
TST is not adequate for the diagnosis of latent TB in populations with high BCG coverage and/or high level of NTM exposure (5,13,14). Eum et al. reported that TST is likely to be a good indicator of latent infection in a population of BCG- unvaccinated subjects but it is confounded with BCG vaccination (15). Many reports indicate that BCG vaccination affects TST in diagnosis of TB infection (5,13,14), others report controversial data. Pai et al. and Dogra et al. showed a high concordance between TST and QTF either in health care workers or in children in India, suggesting there is little influence of BCG vaccination on TST (16,17). However their study population consisted of only once injection of BCG at birth. Floyd et al. reported that repeat vaccinations have more persistent effect on TST (18). In our study, there was a statistically significant relation between the number of BCG scars and the diameter of TST. TST result of HCWs with two BCG scars were significantly higher than HCWs without a BCG scar.
Many reports showed that QTF is not affected by previous BCG vaccinations (5,6,19,20). We also found that, QTF results according to previous BCG vaccinations did not significantly differ. The clinical importance of this is that QTF-GIT test can be an alternative to TST in BCG vaccinated individuals.
Pottumarty et al. compared TST and QTF test results and showed a significant and intermediate correlation between two tests. In our study, there was a statistically significant and a positive correlation of 40% between TST and QTF-GIT assay. We grouped the TST results into 0-4 mm, 5-9 mm, 10-15 mm and > 15 mm. When TST is > 10 mm, QTF-GIT test result was 91.2% positive. This shows that if, TST is > 10 mm, it is most likely that QTF is positive.
Mazurek et al. compared TST and QTF test results in a study population of 1226 people that they grouped into 4 according to TB risk. Group 1 composed of people with no known risk factor for TB, group 2, with high risk for latent TB, group 3, people under investigation for TB and group 4 that have been diagnosed as having culture proven TB before. Concordance in group 1 was 91.8% (n= 98, k= 0.14), in group 2, 84.9% (n= 947, k= 0.55), in group 3, 78.7% (n= 94, k= 0.41) and group 4, 69% (n= 56, k= 0.55). Concordance was 65% when TST was positive (QTF is also positive) and 90% when TST was negative (QTF is also negative) (5). Pai et al. in their study conducted in India on 719 health care workers, reported a concordance of 81% (TST >10 mm) between TST and QTF. This concordance was 80.4% in BCG vaccinated population (16). There was an intermediate concordance between QTF-GIT and TST in our study. We attributed this intermediate concordance to our routine BCG vaccination programme.
Pai et al. reported that years served in the health care profession (> 5 vs. ≤ 1 years) had a statistically significant effect on both TST and QTF results (16). In the present study, number of years in the health care profession significantly affected the QTF-GIT test results. However, number of years in the health care profession did not significantly affect the TST result. Job category (nurse, orderly) and duration of years in the health care profession (1-5 years) were significantly associated with latent tuberculosis infection.
In conclusion, TST is affected by previous BCG vaccinations, while QTF-GIT is not. We suggest that QTF-GIT test can be used as an alternative to TST for the detection of LTBI in populations with routine BCG vaccination programme.
CONFLICT of INTEREST
None declared.
REFERENCES
- Corbett EL, Watt CJ, Walker N, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med 2003; 163: 1009-21. [?zet] [Tam Metin] [PDF]
- World Health Organization. Global Tuberculosis Control. Surveillance, Planning, Financing: WHO Report 2005. Geneva: World Health Organization, 2005:1-247.
- Menzies D, Fanning A, Yuan L, et al. Tuberculosis among health care workers. N Engl J Med 1995; 332: 92-8.
- Jensen PA, Lambert LA, Iademarco MF, et al. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005.
- Mazurek GH, LoBue PA, Daley CL, et al. Comparison of a whole blood interferon gamma assay with tuberculin skin testing for detecting latent mycobacterium tuberculosis infection. JAMA 2001; 286: 1740-7. [?zet] [Tam Metin] [PDF]
- Kipfer B, Reichmuth M, B?chler M, et al. Tuberculosis in a Swiss army camp: caontact investigation using an Interferon gamma release assay. Swiss Med Wkly 2008; 138: 267-72. [?zet] [PDF]
- Lalvani A, Richeldi L, Kunst H. Interferon gamma assays for tuberculosis. Lancet Infect Dis 2005; 5: 322-4.
- American Thoracic Society. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med 2000; 161: 221-47. [PDF]
- Pai M, Joshi R, Dogra S, et al. Serial testing of health care workers for tuberculosis using interferon gamma assay. Am J Respir Crit Care Med 2006; 174: 349-55. [?zet] [Tam Metin] [PDF]
- Pottumarthy S, Morris AJ, Harrison AC, et al. Evaluation of the tuberculin gamma interferon assay: potential to replace the mantoux skin test. J Clin Microbiol 1999; 37: 3229-32. [?zet] [Tam Metin] [PDF]
- Menzies D. What does tuberculin reactivity after Bacille Calmette-Guerin vaccination tell us? Clin Infect Dis 2003; 31 (Suppl 3): S71-4. [?zet] [Tam Metin] [PDF]
- Mazurek GH, Jereb J, Lobue P, et al. Guidelines for using the QuantiFERON-TB Gold test for detecting mycobacterium tuberculosis infection, United States. MMWR Recomm Rep 2005; 54: 49-55. [?zet] [Tam Metin]
- Andersen P, Munk ME, Pollock JM, et al. Specific immune-based diagnosis of tuberculosis. Lancet 2000; 356: 1099-104. [?zet]
- Ewer K, Deeks J, Alvarez L, et al. Comparison of T-cell-based assay with tuberculin skin test for diagnosis of Mycobacterium tuberculosis infection in a school tuberculosis outbreak. Lancet 2003; 361: 1168-73. [?zet]
- Eum SY, Lee YJ, Kwak HK, et al. Evaluation of the diagnostik utility of a whole blood interferon gamma assay for determining the risk of exposure to Mycobacterium tuberculosis in BCG-vaccinated individuals. Diagn Microbiol Infect Dis 2008; 61: 181-6. [?zet] [Tam Metin] [PDF]
- Pai M, Gokhale K, Joshi R, et al. Mycobacterium tuberculosis infection in health care workers in rural India: comparison of a whole blood interferon gamma assay with tuberculin skin testing. JAMA 2005; 293: 2746-55. [?zet] [Tam Metin] [PDF]
- Dogra S, Narang P, Mendiratta DK, et al. Comparison of a whole blood interferon gamma assay with tuberculin skin testing for the detection of tuberculosis infection in hospitalized children in rural India. J Infect 2007; 54: 267-76. [?zet]
- Floyd S, Ponnighaus JM, Bliss L, et al. Kinetics of delayed type hypersensitivity to tuberculin induced by bacille Calmette-Guerin vaccination in northern Malawi. J Infect Dis 2002; 186: 807-14. [?zet] [Tam Metin] [PDF]
- Dominguez J, Manzano JR, Galvao MDS, et al. Comparison of two commertially available gamma interferon blood tests for immunodiagnosis of tuberculosis. Clinical and Vaccine Immunology 2008; 15: 168-71. [?zet] [Tam Metin] [PDF]
- Brock I, Weldingh K, Lillebaek T, et al. Comparison of tuberculin skin test and new specific blood test in tuberculosis contacts. Am J Respir Crit Care Med 2004; 170: 65-9. [?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Ebru DAMADO?LU,
Ba?lar Caddesi G?ven Apartman?
No: 71/5 Seyranba?lar? ANKARA - TURKEY
e-mail: edamadoglu@yahoo.co.uk