Kayseri ilinde kot a?artma i?inde ?al??an i??ilerde mesleki ast?m prevalans?
Nuri TUTAR, Ramazan DEM?R, Hakan B?Y?KO?LAN, Fatma Sema OYMAK, ?nci G?LMEZ, Asiye KANBAY
Erciyes ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Kayseri.
?ZET
Kayseri ilinde kot a?artma i?inde ?al??an i??ilerde mesleki ast?m prevalans?
Kot a?artma i?lemi, kot kumlama i?leminin silikozise neden oldu?unun saptanmas?ndan sonra kotu beyazlatmak i?in kullan?lan en s?k y?ntemdir. Bu ?al??man?n amac?; Kayseri ilinde kot a?artma i?inde ?al??an i??ilerde mesleki ast?m prevalans?n? saptamakt?r. ?al??ma Aral?k 2008-?ubat 2009 tarihleri aras?nda Kayseri ilinde kot a?artma i?leminin yap?ld??? d?rt fabrikada yap?ld?. ?al??maya a?artma b?l?m?nde ?al??an 21, di?er b?l?mlerde ?al??an 22 i??i al?nd?. Kat?l?mc?lara solunumsal semptomlar? da i?eren bir anket uyguland?. Solunum fonksiyon testi (SFT) ve tepe ak?m h?z? (PEF) takibi yap?ld?. T?m kat?l?mc?lara posteroanterior akci?er grafisi ?ekildi. Mesleki ast?m prevalans? a?artma i?inde ?al??anlarda %23.8, di?er b?l?m i??ilerinde ise %9.1 olarak bulundu (p> 0.05). ???ilerde en s?k saptanan semptomlar egzersizde nefes darl??? (%23.3) ve h???lt?l? solunum (%20.9) idi. Kot a?artma i?inde ?al??ma s?resi ile SFT aras?nda ili?ki olup olmad??? kot a?artma i??ilerinde (n= 21) incelendi?inde FEV1 ve FEF25-75 ile orta derecede (s?ras?yla r= -0.477, -0.449); FEV1% ve FEV1/FVC ile iyi derecede (s?ras?yla r= -0.588, -0.509), ters y?nde ve istatistiksel olarak anlaml? ili?ki saptand? (p< 0.05). Sonu? olarak; kot a?artma ajanlar?na maruz kalma solunumsal semptomlar?n ortaya ??kmas?nda, solunum fonksiyonlar?n?n azalmas?nda ve mesleki ast?m olu?umunda ?nemli rol oynamaktad?r.
Anahtar Kelimeler: Kot a?artma, mesleki ast?m.
SUMMARY
The prevalence of occupational asthma among denim bleachery workers in Kayseri
Nuri TUTAR, Ramazan DEM?R, Hakan B?Y?KO?LAN, Fatma Sema OYMAK, ?nci G?LMEZ, Asiye KANBAY
Department of Chest Diseases, Faculty of Medicine, Erciyes University, Kayseri, Turkey.
The bleachery procedure is the most frequent method used to decolorize denims since sandblasting has been shown to cause silicosis. The aim of this study was to determined the prevalence of occupational asthma among denim bleachery workers in Kayseri. The study was conducted in 4 factories, in which jean bleachery was performed, in Kayseri between December 2008 and February 2009. Overall, forty-four subjects, 22 from the bleachery section and 22 from the other sections, were included. A questionnaire about respiratory symptoms was administered. Pulmonary function tests (PFTs) and serial peak expiratory flow (PEF) measurements were performed. All subjects were evaluated by posteroanterior chest x-rays. The prevalence of occupational asthma (OA) in the bleachery and other section workers was 23.8% and 9.1%, respectively (p> 0.05). Within workers, exercise dyspnea (23.3%) and wheezing (20.9%) were the most frequent symptoms. The relationship between the duration of employment and PFTs in bleachery workers (n= 21) was negatively correlated and statistically significant with FEV1, FEF25-75 (moderate; r= -0.477, -0.449, respectively; p< 0.05) and FEV1/FVC, FEV1% (well; r= -0.588, -0.509, respectively; p< 0.05). The results of the present study suggest that exposure to denim-bleaching agents plays an important role in the occurrence of respiratory symptoms, reduction in pulmonary functions, and induction of occupational asthma.
Key Words: Denim bleaching, occupational asthma.
Despite a significant decreasing trend of most occupational respiratory system diseases, especially pneumoconiosis in countries where primary prevention measures are regularly executed, the prevalence of occupational asthma (OA) is rising (1). The major cause of this problem is the constant introduction of several new substances with unknown short and long-term effects in work settings (1). The longitudinal studies indicate that 16.3% of all adult-onset asthma caused by occupational exposures (2).
The number of substances currently known to cause occupational asthma exceeds 400 (3). The bleachery procedure is a method used to decolorize denims. The bleaching procedure involves the use of several chemical agents, including sodium hypochlorite (NaOCl) and potassium permanganate (KMnO4). When inhaled in high concentrations, NaOCl may lead to reactive airway dysfunction syndrome (RADS) (4,5). NaOCl has also been shown to cause occupational asthma in paper factory and pool workers (6,7). However, there are no reports in the literature showing that KMnO4 inhalation, which is used in metal cleaning and fabric bleaching, causes occupational asthma.
The aim of this study was to determine the prevalence of occupational asthma among denim bleacheary workers and to determine if this field of work is a risk factor for occupational asthma.
MATERIALS and METHODS
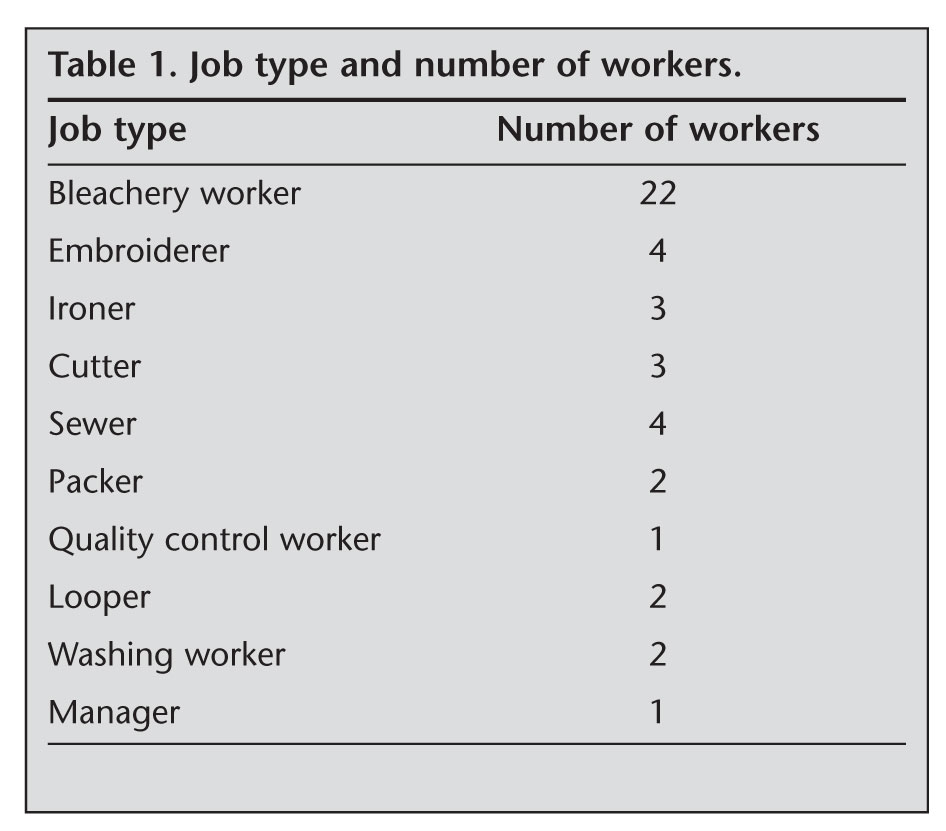
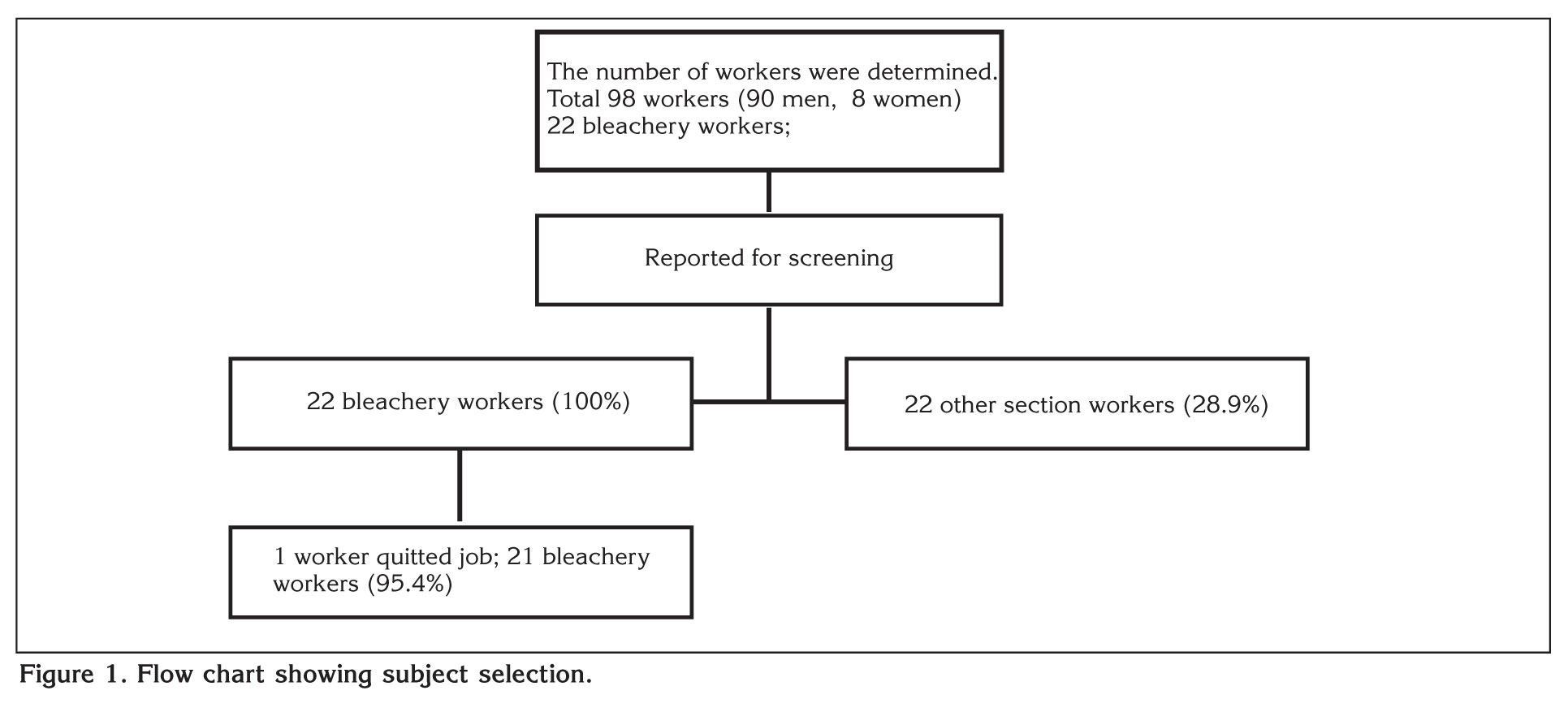
The study was conducted in 4 factories, in which denim bleaching was performed, in Kayseri, Turkey between December 2008 and February 2009. In all four factories, KMnO4 was primarily used during bleaching while NaOCl was used in rare occasions when further decolorization of the product was desired. While bleaching was performed by spray guns in one factory, brushing was used in the other factories. Bleaching was performed in a separate section in one factory, while there were connections between all sections in the other three. Total 98 employees were working in 4 factories. All of the 22 bleachery workers (100%) were included the study. 22 employees (28.9%) were selected in other sections at random (Table 1). Overall, forty-four subjects were included. As one employee working in the bleaching section quitted his job 1 day after being included in the study, the data from 43 employees were analyzed (Figure 1). The 21 subjects working in the bleaching section who had direct contact with the irritant substances were designated as bleachery workers, and the remaining subjects who had indirect contact with the irritants were designated as other section workers.
Questionnaire
A questionnaire form which was developed by the European Community Respiratory Health Survey (ECRHS), and modified by Vandenplas et al., was completed by face-to-face interviews of all subjects (8). Questionnarie includes type of the job, duration of work under the same job, work shift, previous job, previous asthma history and the nature of symptoms during working periods, i.e. chest symptoms (cough, sputum, chest tightness, wheezing, shortness of breath at rest and/or on exertion, change in voice), general symptoms (fever, chills, muscle or joint pain). Information was also obtained on the timing of the onset of symptoms in relation to the beginning of the occupation and the interval between the last occupational exposure and the questionnaire. The relationship between work and respiratory symptoms was also addressed by asking whether symptoms differed on days at work and away from work.
Radiologic Evaluations
All subjects were evaluated by posteroanterior chest X-rays to investigate other respiratory diseases. All X-rays were evaluated by an experienced radiology specialist and the researcher. The subjects with abnormal chest X-ray findings were further evaluated by computed tomography (CT).
Pulmonary Function Tests (PFTs)
PFTs of all subjects were performed using a SensorMedics Vmax 20c device in a sitting position using a nasal clip and were in accordance with the test procedures recommended by the American Thoracic Society (9). At least three measurements were made for each subject, and their best performances were recorded. FVC, FEV1, FEV1/FVC, peak expiratory flow (PEF), and forced expiratory flow 25-75% (FEF25-75) were measured. All measurements were expressed as the percentage of normal values, adjusted for age and height. The test was repeated 15-20 minutes after 400 ?g of salbutamol inhalation in all subjects. A 12% or 200 mL increase in FEV1 or a 20% increase in PEF was considered as positive reversibility.
PEF
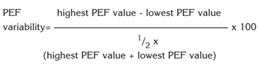
All subjects were informed and trained to use a peak expiratory flow (PEF) meter. They were asked to perform PEF measurements 4 times daily; 3 measurements per each time point (1 at 08:00 before starting work, 2 during work at 10:00 and 15:00, and 1 before leaving work at 18:00) and the best of 3 measurements were recorded at each time for 3 weeks, including weekends (1). All subjects were checked on day 2 to assure that they were using the PEF meter correctly. PEF variability was calculated for each day using the following formula, and the values > 20% were considered to be positive (4):
Diagnosis
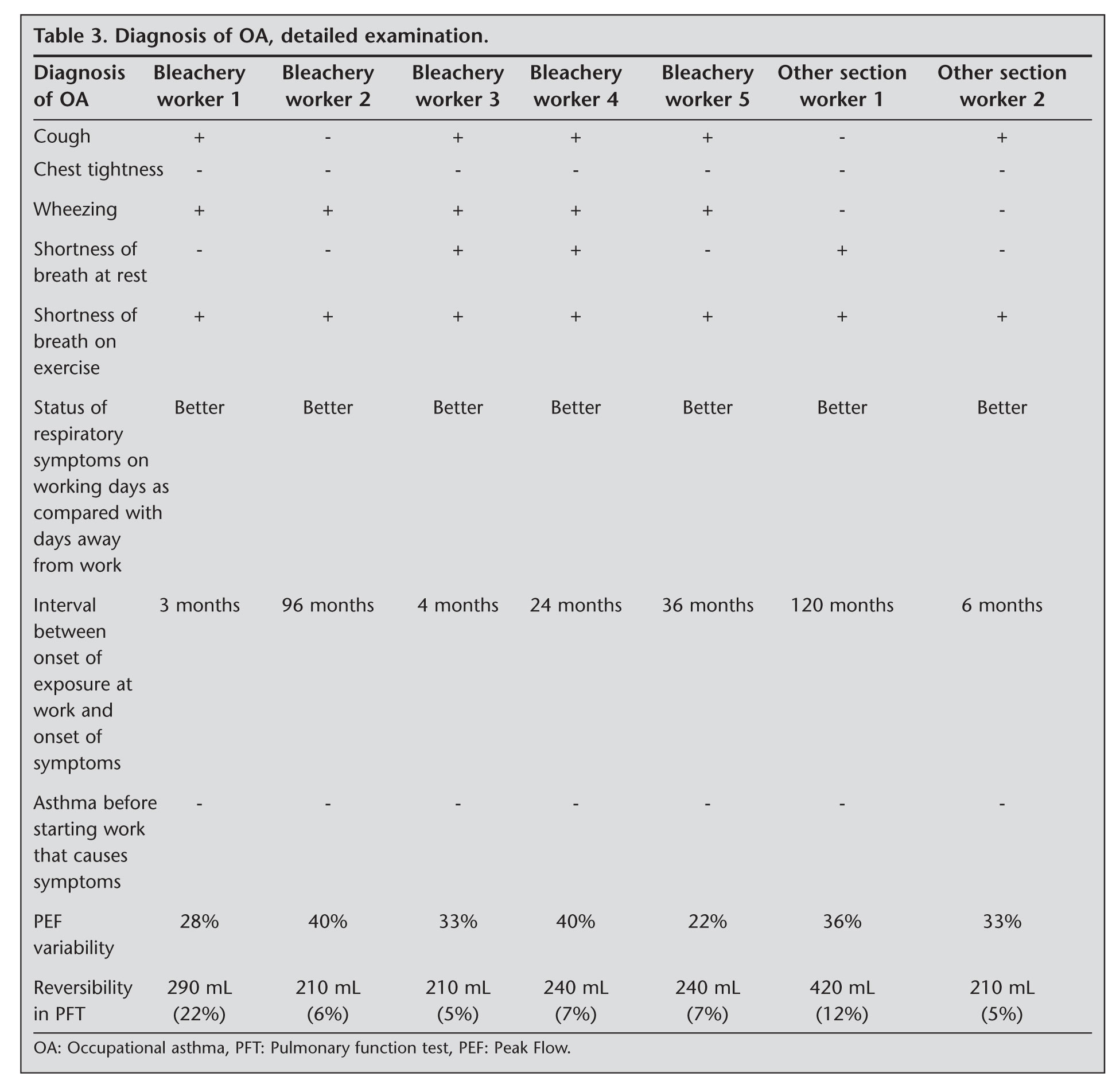
According to American College of Chest Physicians (ACCP) criteria, subjects with one of the asthma symptoms (cough, chest tightness, wheezing, and shortness of breath at rest and following exercise; which were determined by questionnaire) that lessen or disappear when the subject leaves the work environment, with reversibility in PFT plus variability in PEF > 20%, and did not have a history of asthma before their employment, were diagnosed with occupational asthma (4).
Statistical Analysis
All statistical analyses were performed using SPSS 15. Between group comparisons of parametric variables were made by a student's t-test and non-parametric variables by a chi-square test. Pearson correlation analysis was performed to evaluate the correlation between the duration of employment and PFT results. Descriptive analysis of data expressed as mean ? standard deviation (SD), range and percentage, a p value of < 0.05 was used as the level of statistical significance.
RESULTS
Among 43 subjects (39 men and 4 women) included in the study, 21 were bleachery workers and 22 were other section workers. The mean age of bleachery workers was 29.4 ? 6.8 years, and the duration of employment was 32.9 ? 32.3 months. The mean age of the other section workers was 32.5 ? 10.8 years, and the duration of employment was 57.1 ? 70.5 months. There was no significant difference between the two groups in terms of age and duration of employment (p> 0.05).
The smoking status of the workers was as follows: 26 (60.5%) current smokers, 15 (34.9%) never smoked, and 2 past smokers. The total cigarette consumption of the workers was 9.0 ? 9.6 pack years. Fifteen bleachery (71.4%) and 11 other section workers (50%) were current smokers. Two of the bleachery workers were past smokers. The total amount of cigarette consumption of the bleachery and other section workers were 8.1 ? 7.9 and 10.4 ? 12.0 pack years, respectively. There was no significant difference between the two groups in terms of smoking status and the total amount of cigarette consumption (p> 0.05).
Among asthma symptoms, shortness of breath following exercise was present in 10 workers, wheezing in 9, cough in 8, shortness of breath at rest in 4, and chest tightness in 2 workers. When asthma symptoms in the bleachery and other section workers were compared, all asthma symptoms except chest tightness were found to be more frequent in the bleachery workers. No significant difference was observed between the two groups in terms of asthma symptoms (p> 0.05).
The mean FEV1/FVC was 81.7%, the mean FEV1 was 4.0 L (101.8%), and the mean FVC was 4.8 L (104.8%) in all workers. When bleachery and other section workers were evaluated separately, FVC%, FEV1%, FEV1/FVC, PEF, PEF%, FEF25-75, and FEF25-75% values were lower in the bleachery workers, but the difference was not statistically significant (p> 0.05; Table 2).
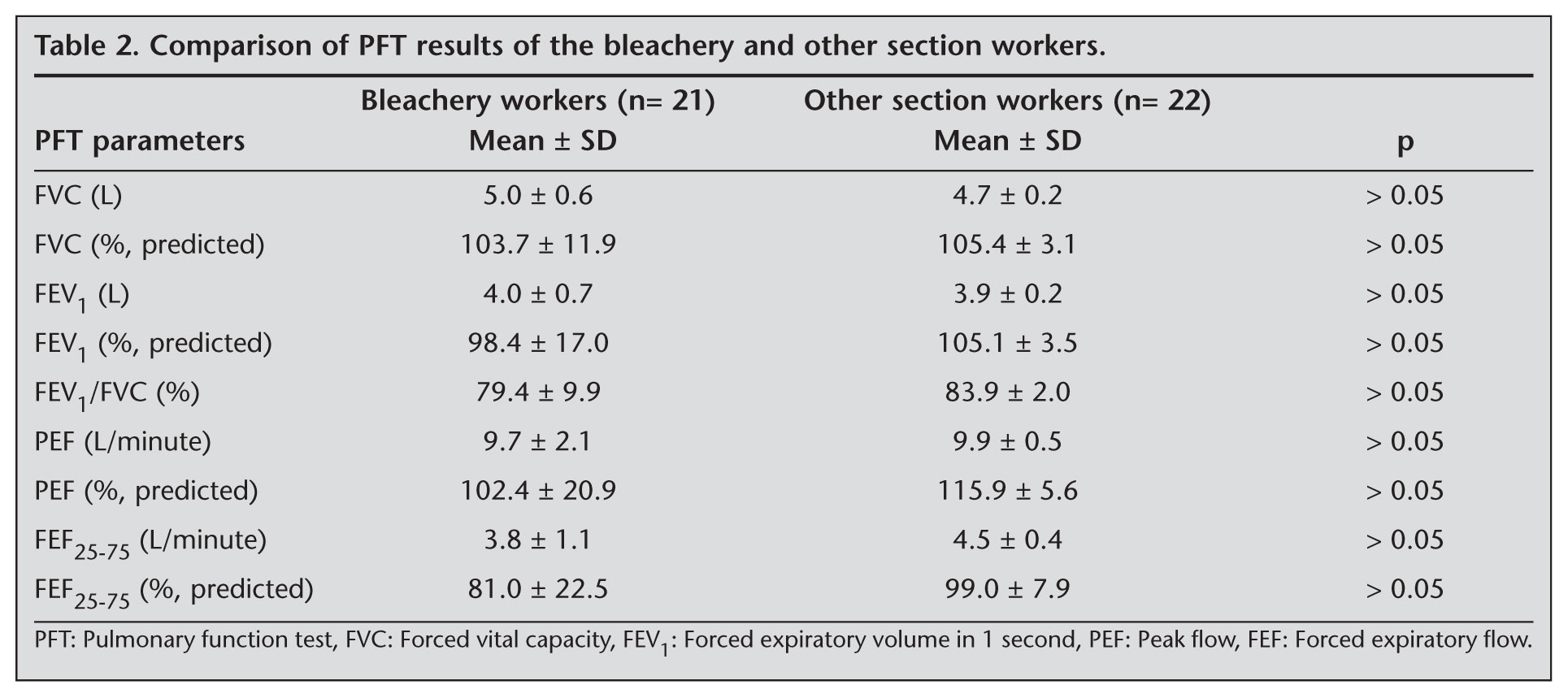
The relationship between the duration of employment and PFTs in bleachery workers (n= 21) was evaluated by Pearson correlation analysis. The duration of employment was negatively correlated and statistically significant with FEV1, FEF25-75 (moderate; r= -0.477, -0.449, respectively; p< 0.05) and FEV1%, FEV1/FVC (good; r= -0.509, -0.588, respectively; p< 0.05).
None of the individuals had an asthma history which diagnosed by a doctor. Seven subjects (16.3%) in the study population, with asthma symptoms (cough, chest tightness, wheezing, and shortness of breath at rest and following exercise) which began after they started to work in their current occupation and lessened or disappeared when they left the work environment, with PFT reversibility plus PEF variability, were diagnosed as occupational asthma according to ACCP criteria (Table 3). Five of the 7 subjects were bleachery workers, with 3 using brushing and 2 using spraying methods. Four of the bleachery workers who were diagnosed with occupational asthma described bleaching as the procedure responsible for their respiratory symptoms. The 2 other section workers with occupational asthma were employed in factories without separate sections, and their work place was close to the place where the bleaching was performed. The prevalence of occupational asthma in the bleachery and other section workers was 23.8% and 9.1%, respectively, and there was no statistically significant difference between the groups (p> 0.05).
The smoking status of workers with occupational asthma was as follows: four asthmatic workers were current smokers, 1 was a past smoker and 2 have never smoked. There was no statistically significant difference between subjects with or without occupational asthma, in terms of smoking status (p> 0.05).
When subjects with (n= 7) or without (n= 36) occupational asthma were compared, FVC%, FEV1, FEV1%, FEV1/FVC, PEF%, FEF25-75, and FEF25-75% values were lower in the asthma group. There was a statistically significant difference between the groups in terms of FEV1/FVC and FEF25-75% values (p< 0.05). Also PEF variability in workers with or without occupational asthma was 33.1% and %11.7, respectively, and the difference was statistically significant (p< 0.05).
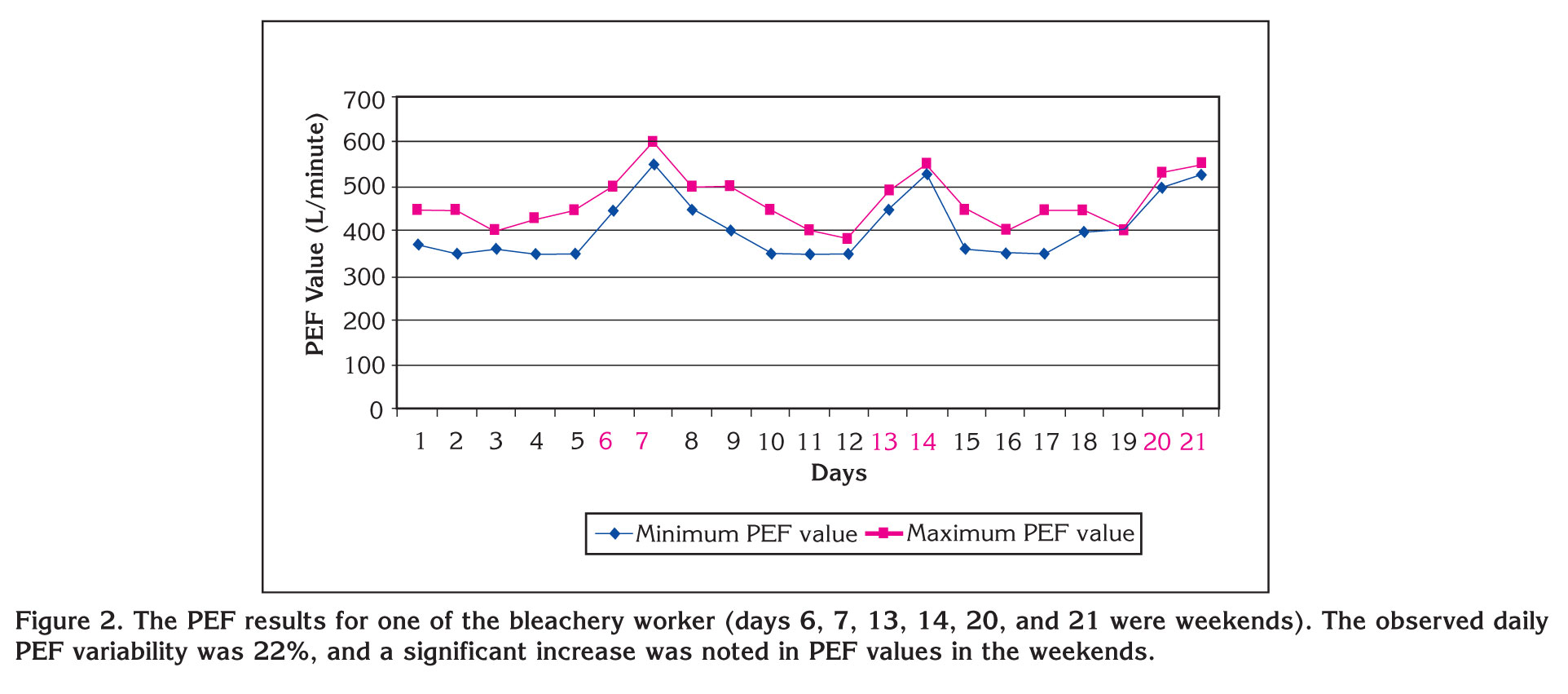
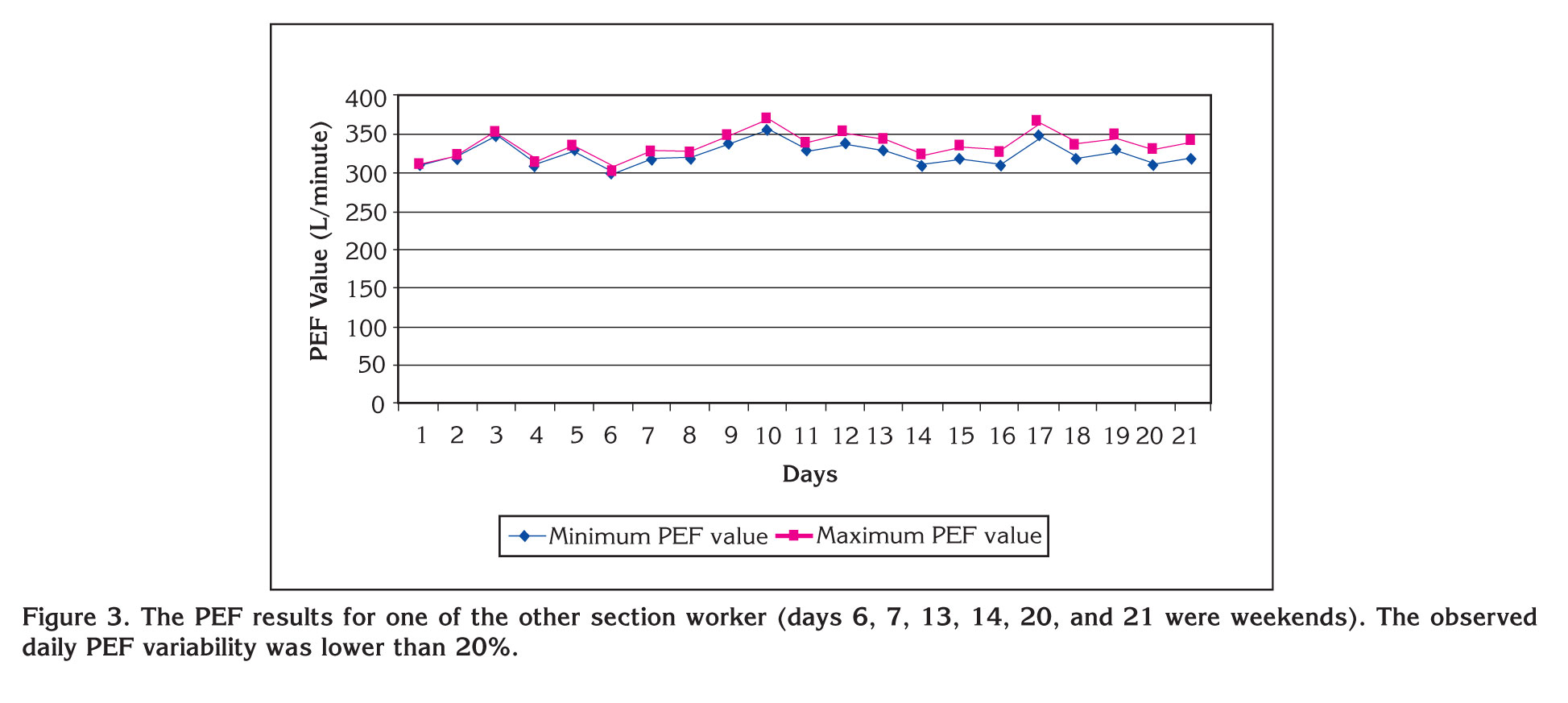
The PEF results of two subjects with or without occupational asthma are presented in Figures 2,3.
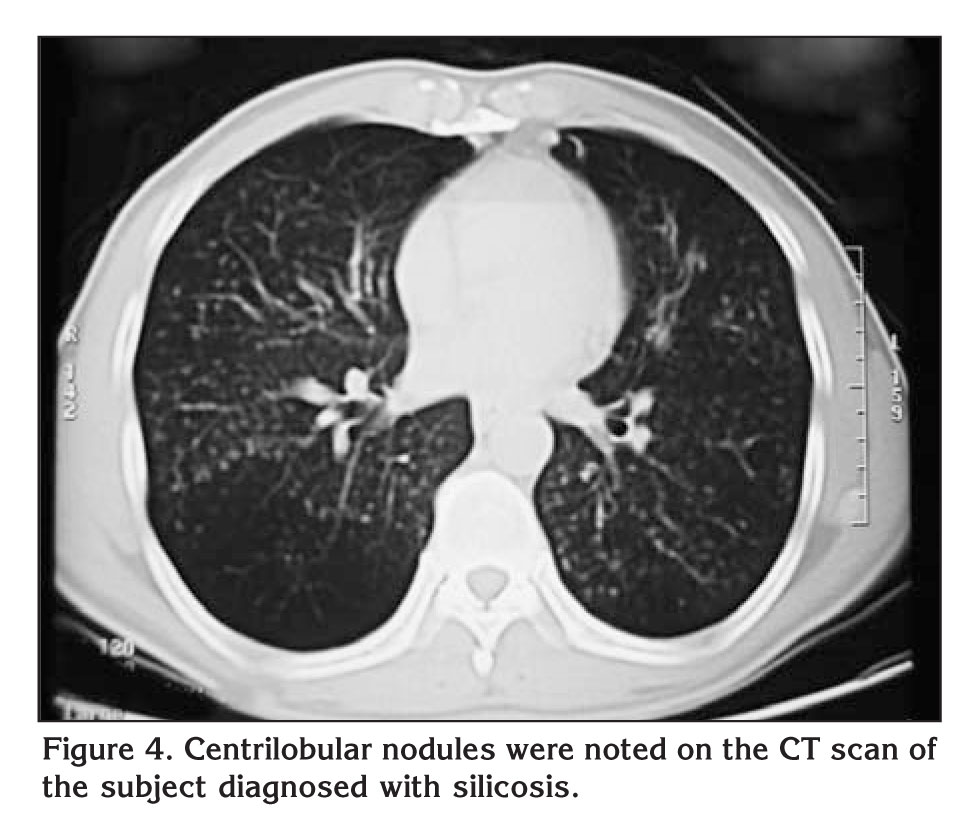
One of the posteroanterior chest X-ray evaluation of the bleachery workers revealed a reticulonodular pattern. He was further evaluated by computed tomography and mediastinal lymph nodes were noted. Parenchymal evaluation revealed centrilobular nodules in both lungs, especially prominent in the upper and middle lobes (Figure 4). The PFT results of the subject were as follows: FEV1/FVC, 41%; FEV1, 1.31 L (34%); FVC, 3.17 L (70%); and FEV1 reversibility, 290 mL (22%). When the subject's occupational history of sandblasting for 4 years beginning 10 years ago was taken into account, the worker was diagnosed with silicosis.
DISCUSSION
Occupational asthma has been reported to be associated with several occupation groups in the literature, including automobile and furniture painters, hairdressers, bakers, paper factory workers, carpenters and furniture makers, florists, healthcare staff, and carpet factory workers (10).
Occupational asthma may be observed in paper factory workers exposed to NaOCl, sodium sulphate, alkaline soda, and sulphur compounds. Orman et al. reported the prevalence of occupational asthma in paper factory workers to be 3.1% (6). Low molecular weight agents, particularly isocyanate, may cause occupational asthma in automobile and furniture painters (11). In a study conducted in Eskisehir, the prevalence of occupational asthma in automobile and furniture painters was 9.6% (12).
The diagnosis of occupational asthma is based on the presence of a specific agent, which is known to cause asthma, in the workplace, the presence of asthma symptoms, and the demonstration of a causal relationship with this agent. The most common method used to identify this relationship is PEF monitoring. It has been suggested that respiratory questionnaires and PEF monitoring may be good alternatives to nonspecific bronchial provocation test (NSBPT), to demonstrate airway hyperreactivity in practice (13). Although NSBPT has been recommended to be used in the diagnosis of occupational asthma, certain limitations of the test have also been stated as it requires experienced staff and can be performed in specific centers (14,15). In two studies involving furniture and automobile painters, it has been suggested that a detailed occupational and respiratory system history should be obtained for the diagnosis of occupational asthma, and serial PEF monitoring is appropriate to demonstrate the symptom-workplace connection in Turkey where NSBPT is not widely available (16,17). Patient related factors such as respiratory infection within the 6 weeks prior to testing, and gastroesofageal reflux disease can impact the NSBPT results (4). Furthermore, Leroyer et al. have found that sensitivity and specificity of PEF monitoring is higher than FEV1 monitoring (18).
Our study involved 43 workers in 4 different factories. Seven subjects (16.3%) with asthma-like symptoms related to working hours, PFT reversibility, and PEF variability were diagnosed as occupational asthma according to ACCP criteria. The prevalence of occupational asthma was 23.8% (n= 5) in bleachery workers and 9.1% (n= 2) in other section workers. The condition of 2 workers working in the factories where bleaching was not performed in a separate section was thought to be related to occupational asthma rather than classical asthma, as their workplaces were close to the bleaching section, the PEF variability was normal in the weekends, and the asthma symptoms appeared after starting work. Although we have observed no statistically significant difference between these two groups (p> 0.05), our results suggest that the prevalence of occupational asthma and the likelihood of the bleaching procedure to cause occupational asthma is higher in bleachery workers compared to other section workers in the factory. However, employees working close to the bleaching section might also be at risk for occupational asthma. It has to be noted that occupational asthma has not been observed in any of the 7 other section workers employed in factories where the bleaching procedure is performed in a separate section. Respiratory symptoms associated with agents used in the denim-bleaching procedure have been described in previous studies; however, this occupation has not been defined as a risk factor for occupational asthma (5,6,7,19,20,21). Our results suggest that a history of employment in factories where jean bleaching is performed (especially in the bleaching section) should be investigated in patients suspected of occupational asthma.
It is well-known that a reduction in FEV1/FVC and FEV1 is an indicator of obstructive abnormalities, and that a reduction in FEF25-75 is an indicator of small airway obstruction (22). In a controlled study involving 166 workers exposed to sodium sulphate, alkaline soda, sulphur compounds, chlorine, chlorine dioxide in a paper factory, FEV1 and FEV1%, FVC and FVC%, FEF25-75 and FEF25-75%, and FEV1/FVC values were lower in the workers compared to controls, and the differences between the groups in terms of FEV1/FVC, FEV1/FVC%, and FEV1% were statistically significant (22). In a Swedish study involving paper factory workers exposed to chlorine dioxide and sulphur dioxide, PFT was monitored for 3 years in certain intervals and the reductions in FEV1 and FVC, was associated with the duration of employment (23). In our study the PFT results of workers with or without occupational asthma were compared, FVC%, FEV1, FEV1%, FEV1/FVC, PEF%, FEF25-75, and FEF25-75% were lower in the occupational asthma group. A statistically significant difference was noted between the two groups regarding FEV1/FVC and FEF25-75% values. The significantly lower FEV1/FVC and FEF25-75% observed in the occupational asthma group was in accordance with the expected PFT results in asthma. Moreover, when the correlation between PFT results and the duration of substance exposure was evaluated, a negative correlation was observed between the duration of substance exposure and FEV1% and FEV1/FVC (good correlation), and FEV1 and FEF25-75 (moderate correlation). These results indicated that the duration of substance exposure in workers involved in denim-bleaching was associated with a low FEV1 and a reduction in FEF25-75, indicators of small airway obstruction, as expected in asthma and was moderately correlated with low FEV1/FVC, another indicator of obstruction.
In this study KMnO4 was frequently and NaOCL was rarely used for bleaching. Particularly, exposure to high doses of NaOCL is associated with reactive airways dysfunction syndrome (RADS) and chronic exposure to this substance may lead to irritant-induced asthma (IIA) in paper factory workers and pool workers (7,24,25). To our knowledge, there are no studies in the literature evaluating occupational asthma related to KMnO4 exposure. Frequent exposure of employees to KMnO4 and occurrence of respiratory symptoms after a mean period of 32 months (range, 3-120 months) in our study suggest an incidence of irritant-induced occupational asthma. But the study population is too small and given some lack of statistical significance. So the exact relationship between KMnO4 exposure and occupational asthma can only be determined by further studies comparing employees with exposure to KMnO4 alone and control subjects with no exposure to the potential causative agent.
CONCLUSION
In conclusion, this article suggests that exposure to denim-bleaching agents plays an important role in the occurrence of respiratory symptoms, reduction in pulmonary functions, and induction of occupational asthma. Silicosis should also be considered in employees with a previous occupational history of sandblasting.
CONFLICT of INTEREST
None declared.
REFERENCES
- Akkurt ?. Occupational respiratory disease. 1st ed. Ankara: Turkish Medical Association Press, 2007: 62-70.
- Toren K, Blanc P. Asthma caused by occupational exposures is common- A systematic analysis of estimates of the population- attributable fraction. BMC Pulmonary Journal 2009; 9.
- Bernstein IL, Chan-Yeung M, Malo JL, Bernstein DI. Definition and classification of asthma in the workplace. In: Bernstein IL, Chan-Yeung M, Malo JL, Bernstein DI (eds). Asthma in the Workplace. 3rd ed. New York: Taylor & Francis, 2006: 1-8.
- Tarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bersntein D, et al. Diagnosis and management of work-related asthma: American College of Chest Physicians Consensus Statement. Chest 2008; 134 (Suppl 3): 1-41. [?zet] [Tam Metin] [PDF]
- D'Alessandro A, Kuschner W, Wong H, Boushey BA, Blanc PD. Exaggerated responses to chlorine inhalation among persons with nonspecific airway hyperreactivity. Chest 1996; 109: 331-7. [?zet]
- Orman A, Ellidokuz H, Esme H, ?nl? M, Ay A. Evaluation of pulmonary system symptoms with pulmonary functional tests in workers in pulp and paper industry. Respiratory Diseases 2004; 15: 165-9.
- Thickett KM, McCoach JS, Gerber JM, Sadhra S, Burge PS. Occupational asthma caused by chloramines in indoor swimming-pool air. Eur Respir J 2002; 19: 827-32. [?zet] [Tam Metin] [PDF]
- Vandenplas O, Ghezzo H, Munoz X, Moscato G, Perfetti L, Lemiere C, et al. What are the questionnaire items most useful in identifying subjects with occupational asthma? Eur Respir J 2005; 26: 1056-63. [?zet] [Tam Metin] [PDF]
- Standardization of spirometry -- 1987 update: statement of the American Thoracic Society. Am Rev Respir Dis 1987; 136: 1285-98.
- From the Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA) Updated 2007. (Accessed February 10, 2010 at: http://sichon.wu.ac.th/ file/pharmacy-20081207-154031-14Lwl.pdf )
- Park HS, Nahm DH. Isocyanate-induced occupational asthma: challenge and immunologic studies. Korean Med Sci 1996; 11: 314-8. [?zet] [PDF]
- Ucgun I, Ozdemir N, Metintas M, Metintas S, Erginel S, Kolsuz M. Prevalence of occupational asthma among automobile and furniture painters in the center of Eskisehir (Turkey): the effects of atopy and smoking habits on occupational asthma. Allergy 1998; 53: 1096-100. [?zet]
- Burge PS, O'Brien IM, Harries MG. Peak flow rate records in the diagnosis of occupational asthma due to isocyanates. Thorax 1979; 34: 317-23. [?zet] [PDF]
- Cartier A. Definition and diagnosis of occupational asthma. Eur Respir J 1994; 7:153-60. [?zet]
- Banks DE, Tarlo SM, Masri F, Rando RJ, Weissman DN. Bronchoprovocation tests in the diagnosis of isocyanate-induced asthma. Chest 1996; 109: 1370-9. [?zet] [PDF]
- Turgut T, Ta?demir C, Muz MH, Deveci F, Kirkil G. The prevalence of occupational asthma in auto and furniture dye workers in Elazig downtown. Tuberk Toraks 2005; 53: 371-8. [?zet] [PDF]
- U?gun I, ?zdemir N, Metinta? M, Erginel S, Kolsuz M. The place of peak expiratory flow monitoring in diagnosing occupational asthma in car and furniture painters in the centre of Eskisehir. Tuberk Toraks 2000; 48: 295-300. [?zet] [PDF]
- Leroyer C, Perfetti L, Trudeau C, L'Archev?que J, Chan-Yeung M, Malo JL. Comparison of serial monitoring of peak expiratory flow and FEV1 in the diagnosis of occupational asthma. Am J Respir Crit Care Med 1998; 158: 827-32. [?zet] [Tam Metin] [PDF]
- Stellman JM. Encyclopaedia of occupational health and safety. 4th ed. Geneva: International labour office, 1998: 210-1.
- Dart RC. Medical Toxicology. 4th ed. Philadelphia: Williams and Wilkins, 2004: 903-5.
- Susan DS, Rossol M. Overexposure health hazards in pathology. 2nd ed. New York: Allworth Press, 1991: 130-1.
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J 2005; 26: 948-68. [Tam Metin] [PDF]
- Mehta AJ, Henneberger PK, Tor?n K, Olin AC. Airflow limitation and changes in pulmonary function among bleachery workers. Eur Respir J 2005; 26: 133-9. [?zet] [Tam Metin] [PDF]
- Gorguner M, Aslan S, Inandi T, Cakir Z. Reactive airways dysfunction syndrome in housewives due to a bleach-hydrochloric acid mixture. Inhal Toxicol 2004; 16: 87-91. [?zet]
- Henneberger PK, Lax MB, Ferris BG. Decrements in spirometry values associated with chlorine gassing events and pulp mill work. Am J Respir Crit Care Med 1996; 153: 225-31. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Nuri TUTAR,
Erciyes ?niversitesi T?p Fak?ltesi,
Gevher Nesibe Hastanesi,
G???s Hastal?klar? Anabilim Dal?,
KAYSER? - TURKEY
e-mail: drnuritutar@gmail.com