Bron?ektazide hava yolu kolonizasyonu sistemik inflamasyona neden olur mu?
Beg?m Ergan Arsava, L?tfi ??PL?
Hacettepe ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Ankara.
?ZET
Bron?ektazide hava yolu kolonizasyonu sistemik inflamasyona neden olur mu?
Son d?nemde yap?lan ?al??malar kronik obstr?ktif akci?er hastal??? ve ast?m gibi kronik hava yolu hastal?klar?nda e?lik eden bir sistemik inflamatuvar yan?t?n varl???n? g?stermi?tir. Hava yollar?nda kronik bakteriyel kolonizasyon ve buna ikincil hava yolu inflamasyonu ve ilerleyici hava yolu hasar? ile karakterize bir hastal?k olan bron?ektazide, sistemik inflamatuvar yan?t?n var olup olmad??? bilinmemektedir. Bu ?al??mada bron?ektazide hava yolundaki bakteriyel kolonizasyon ve sistemik inflamasyon aras?ndaki ili?kinin de?erlendirilmesi ama?lanm??t?r. Klinik olarak stabil olan bron?ektazi hastalar? (n= 50) ile ya? ve cinsiyete g?re e?le?tirilmi? kontrol grubunda (n= 30) serum inflamasyon parametreleri [beyaz k?re say?s?, eritrosit sedimentasyon h?z?, C-reaktif protein (CRP), fibrinojen, interl?kin-8, t?m?r nekroz fakt?r?-α ve leptin] de?erlendirilmi?tir. Ayr?ca, bron?ektazili hasta grubunda hava yolu bakteriyel kolonizasyonuna g?re alt analiz yap?lm??t?r. Bron?ektazili hasta ve kontrol gruplar? aras?nda serum inflamasyon parametreleri seviyeleri a??s?ndan fark saptanmam??t?r. Ancak bron?ektazili hasta grubu hava yolu bakteriyel kolonizasyonuna g?re de?erlendirildi?inde median (?eyrekler aras? aral?k-?AA) beyaz k?re say?s?, CRP ve fibrinojen seviyeleri hava yolu kolonizasyonu olan hastalarda (n= 14) olmayanlara g?re belirgin derecede y?ksek olarak saptanm??t?r [s?ras?yla 8.2 (6.4-9.5) ve 6.4 (5.8-7.7) x 103/mm3, 0.91 (0.45-1.29) ve 0.42 (0.30-0.77) mg/dL, 433.5 (390.3-490.3) ve 392.0 (327.0-416.0) mg/dL; p< 0.05]. Bu ?al??mada t?m bron?ektazi grubunda, kontrol hastalar? ile kar??la?t?r?ld???nda, sistemik inflamatuvar parametrelerde art?? saptanmam??t?r. Ancak hastalar hava yolunda bakteriyel kolonizasyon varl???na g?re de?erlendirildiklerinde kolonize hastalarda beyaz k?re, CRP ve fibrinojen seviyelerinin y?ksek oldu?u g?zlenmi?tir. Bu bulgular stabil bron?ektazi hastalar?nda geli?en kronik hava yolu kolonizasyonunun sistemik inflamasyona neden olabilece?ini desteklemekedir.
Anahtar Kelimeler: Bron?ektazi, C-reaktif protein, kolonizasyon, fibrinojen, sistemik inflamasyon.
SUMMARY
Does airway colonization cause systemic inflammation in bronchiectasis?
Beg?m Ergan Arsava, L?tfi ??PL?
Department of Chest Diseases, Faculty of Medicine, Hacettepe University, Ankara, Turkey.
Recent evidence suggests the presence of accompanying systemic inflammation in chronic inflammatory airway diseases such as chronic obstructive pulmonary disease and asthma; however little is known regarding the presence of systemic inflammation in bronchiectasis. Although bronchiectasis was initially considered a stationary process, chronic bacterial colonization causes airway inflammation and progressive airway damage. The aim of this study was to determine the level of systemic inflammation in bronchiectasis patients and identify its relationship with colonization. White blood cell (WBC) count, erythrocyte sedimentation rate, serum C-reactive protein (CRP), plasma fibrinogen, interleukin-8, tumor necrosis factor-α and leptin levels were determined in clinically stable bronchiectasis patients (n= 50), and age- and sex-matched controls. Bronchiectasis patients were also analyzed according to colonization in sputum samples. There was no significant difference between bronchiectasis and control groups with respect to inflammatory markers but median (interquartile range-IQR) WBC count, CRP and fibrinogen levels were significantly higher in colonized patients (n= 14) when compared to non-colonized patients [8.2 (6.4-9.5) vs. 6.4 (5.8-7.7) x 103/mm3, 0.91 (0.45-1.29) vs. 0.42 (0.30-0.77) mg/dL, 433.5 (390.3-490.3) vs. 392.0 (327.0-416.0) mg/dL, respectively; p< 0.05]. There was no evidence supporting the presence of systemic inflammation in the overall bronchiectasis group when compared to controls. However, elevated WBC count, CRP and fibrinogen levels in patients with colonization suggest the presence of a systemic inflammatory response in clinically stable bronchiectasis patients with colonization.
Key Words: Bronchiectasis, C-reactive protein, colonization, fibrinogen, systemic inflammation.
Bronchiectasis, a pathological entity characterized by permanent and abnormal dilatation of one or more bronchi, is a common airway disease in developing countries due to increased prevalence of tuberculosis and other respiratory infections (1,2,3,4). The airway pathology observed in bronchiectasis is not a stationary process due to the ongoing local inflammatory response (4,5). The inflammatory response triggered by microbial infection in bronchiectatic areas causes the release of proteolytic enzymes and oxygen radicals from neutrophils. This leads to impairment in mucociliary activity and retaining of secretions, which in turn creates an environment suitable for recurrent bacterial infections and colonization. The repetitive bouts of infection and inflammation create a vicious cycle, which in end cause progressive damage in the airways (4,5,6).
Previous studies have shown the presence of intense inflammatory activity characterized by neutrophils, T-cells and interleukin (IL)-8 positive cells and elevated levels of IL-6, IL-8, tumour necrosis factor (TNF)-α, leukotriene B4, endothelin 1, elestase in sputum and bronchoalveolar lavage samples of bronchiectasis patients (7,8,9,10,11,12). Recent evidence suggests the presence of systemic inflammation in chronic inflammatory airway diseases. Studies performed in patients with asthma and chronic obstructive pulmonary disease (COPD) have shown elevated levels of systemic inflammatory markers (13,14); however little is known regarding systemic inflammatory response in bronchiectasis (15).
In this study our objective was to determine the levels of systemic inflammatory markers in clinically stable bronchiectasis patients and identify its relationship with airway colonization.
MATERIALS and METHODS
Study Population
We included a consecutive series of patients with an established or new diagnosis of bronchiectasis confirmed by high-resolution computerized tomography (HRCT). The study was performed in a university hospital between January and December 2005. We only included clinically stable patients. "Clinically stable" was defined as 1) absence of any change in respiratory symptoms (increased dyspnea, increased sputum production, change in sputum color), 2) absence of any new respiratory symptoms like cough, dyspnea, hemoptysis, 3) absence of any change in medications, and 4) absence of hospital admission, within six weeks prior to the study. Patients with exacerbations (defined as clinical worsening with increased symptoms like cough, dyspnea, sputum production and increased sputum volume), diagnosis of a systemic disease which may be associated with bronchiectasis (COPD, bronchial asthma, cystic fibrosis, sarcoidosis, interstitial fibrosis, allergic bronchopulmonary aspergillosis) and concurrent use of any medications that may influence systemic inflammation (immunosupressive drugs or systemic corticosteroids) were excluded from the study. A consecutive series of healthy volunteers without any evident airway disease were enrolled into the study as the control group. The study was approved by the local institutional review board and a written informed consent was obtained from all study participants.
Data Collection
Baseline demographic and clinical [age, gender, height, weight, body mass index (BMI), smoking history] data were collected from all study participants. Bronchiectasis group was also reviewed for the type and duration of symptoms, time of diagnosis, possible risk factors for bronchiectasis, and ongoing treatments for bronchiectasis.
HRCT scans of the bronchiectasis patients were evaluated independently by two radiologists and a pulmonologist. The extent of bronchiectasis was evaluated for each lobe individually; lingula was considered as a separate lobe (16).
Lung Function
Forced expiratory volume in one second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio were measured by spirometer (Spirolab II, Medical International Research-MIR, Italy) using standard protocols. Lung function was expressed as both actual and percentage of reference values (17).
Laboratory Analysis
White blood cell (WBC) count, erythrocyte sedimentation rate (ESR), serum C-reactive protein (CRP), immunoglobulin G, A, M and E, and plasma fibrinogen levels were determined in all subjects. Venous blood samples were centrifuged at 3000 rpm and plasma was collected to be stored at -70?C. IL-8 and TNF-α levels were determined by enzyme linked immunosorbent assay (ELISA) and leptin levels were determined by solid phase enzyme amplified sensitivity immunoassay (BioSource International Inc, California, USA). All samples were tested twice and the mean value was used in further analyses.
Microbiological Analysis
Every patient was asked to give sputum samples for quantitative culture at least twice. The quality of specimen was screened by Gram stain; specimens with > 25 leukocytes and < 10 epithelial cells per examination field (x100 magnification) were considered as acceptable. Samples were diluted with an equal volume of 0.9% NaCl solution and vortex mixed for five minutes. Once homogenised, the samples were left for five minutes at room temperature and then ten-fold serial dilutions of sputum samples were plated on blood and haemophilus test medium agars (BD diagnostic system). The cultures were evaluated for growth after 24 and 48 hours. Negative bacterial cultures were discarded after five days. Growth with potentially pathogen microorganisms (Haemophilus influenzae and parainfluenzae, Streptococcus pneumoniae, Moraxella catarrhalis, Pseudomonas aeruginosa, enterobacteria) were considered as positive culture growth and colonization was defined as the presence microorganism growth with ≥ 1 x 105 colony-forming units per milliliter (18,19,20).
Statistical Analysis
All numerical variables are expressed as median (inter-quartile range, IQR). Continuous variables were compared by Mann-Whitney U test and categorical variables were compared by Chi-Square test. Spearman's correlation test was used to assess the relationship between two continuous variables. A two-tailed p value of < 0.05 was considered significant. All statistical analyses were performed using SPSS 14.0.
RESULTS
A total of 50 patients [34 females, 16 males; median (IQR) age: 51.0 (43.0-60.3) years] and 30 controls [18 females, 12 males; median (IQR) age: 47.0 (41.8-59.0) years] were enrolled into the study. The demographic data, clinical characteristics and results of laboratory tests are shown in Table 1.
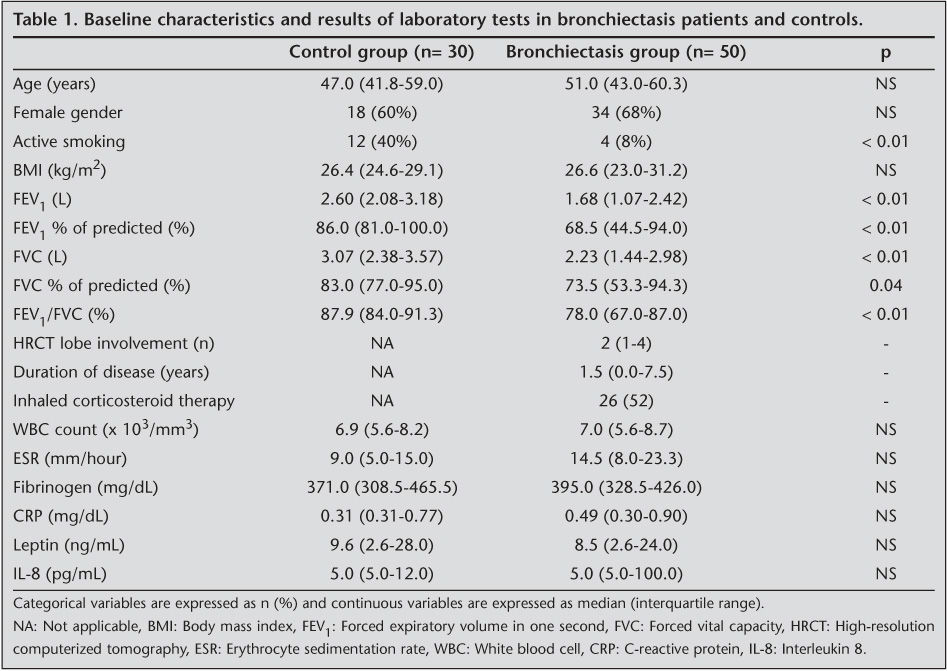
The underlying etiologies considered to be associated with the development of bronchiectasis were as follows: idiopathic (48%), previous tuberculosis infection (26%), post-pneumonic (22%) and primary ciliary dyskinesia (4%). All patients had normal immunoglobulin levels. According to HRCT findings, the median (IQR) number of lobes involved was 2 (1,2,3,4). The patients were followed with a diagnosis of bronchiectasis for a median (IQR) duration of 1.5 (0.0-7.5) years (range: 0-25 years) and none of the patients were on long term prophylactic antibiotic therapy.
When compared to controls, bronchiectasis patients had a lower prevalence of active smoking (8% vs. 40%, p< 0.01). The control group, as expected, had better results in pulmonary function tests. No significant difference was present between patients and controls with respect to levels of inflammatory markers (Table 1). Plasma concentrations of TNF-α remained below the lower detection limit (1.7 pg/dL) in all patients and controls. There was no statistically significant difference for inflammatory markers between patients who were and were not receiving inhaled corticosteroid therapy in the bronchiectasis group. Inflammatory marker levels were similar between smoker and nonsmoker controls.
Thirty-eight (76%) patients were able to give acceptable sputum samples during their clinically stable period; 14 (28%) of these had pathogenic bacterial growth: 8 P. aeruginosa, 4 H. influenzae, 2 S. pneumoniae, 1 M. catarrhalis and 1 H. parainfluenzae. In two patients two different microorganisms grew simultaneously (Pseudomonas aeruginosa and M. catarrhalis; S. pneumoniae and H. influenzae). Patients with colonization had significantly lower FEV1 [1.13 (0.66-2.01) vs. 1.75 (1.19-2.54) liters] and FVC values [1.51 (0.99-2.40) vs. 2.49 (1.52-3.22) liters] when compared to non-colonized patients (Table 2). WBC count, CRP and fibrinogen levels were significantly higher in patients with colonization [8.2 (6.4-9.5) vs. 6.4 (5.8-7.7) x103/mm3, 0.91 (0.45-1.29) vs. 0.42 (0.30-0.77) mg/dL, 433.5 (390.3-490.3) vs. 392.0 (327.0-416.0) mg/dL, respectively].

When patients were categorized according to their sputum culture results, it was seen that P. aeruginosa colonization was associated with older age [70.5 (54.5-76.3) vs. 53.5 (33.8-60.3) years], lower FEV1 [0.83 (0.48-1.5) vs. 1.83 (1.07-2.50) liters], lower FVC [1.20 (0.82-1.78) vs. 2.22 (1.44-3.25) liters], and more diffuse disease [4 (2.5-5.8) vs. 1 (1-3.8) lobes involved] (Table 2). WBC count and fibrinogen levels were higher in P. aeruginosa colonization group [9.0 (7.1-7-9.6) vs. 6.9 (5.8-10.0) x 103/mm3 and 478.0 (431.3-530.0) vs. 378.5 (339.0-429.8) mg/dL]. Patients with P. aeruginosa colonization had higher median leptin levels compared to other patients with bronchial colonization; however this difference did not reach statistical significance [14.7 (0.8-24) vs. 7.3 (0.7-26.1) ng/mL; p> 0.05].
Plasma leptin levels, as expected, were higher in female patients [18.5 (4.9-27.1) vs. 4.4 (0.2-6.8) ng/mL; p< 0.01] and correlated positively with BMI (r= 0.40, p< 0.01). In addition there was a poor but significant correlation between leptin levels and FEV1/FVC ratios (r= 0.30; p= 0.04) but this correlation became insignificant after adjustment for BMI.
DISCUSSION
Permanent dilatation of the airways and impairment of mucociliary clearance result in bacterial colonization in patients with bronchiectasis. Chronic airway infection, in turn, triggers an intense local inflammatory response (12). There is limited data about the presence of a systemic inflammatory component in addition to this local response during the clinically stable period in bronchiectasis (15). In this study, we sought to identify the presence of systemic inflammation in clinically stable bronchiectasis. We measured systemic markers of inflammation in a consecutive series of patients with bronchiectasis and controls. We were not able to find any evidence suggestive of systemic inflammation in the overall bronchiectasis cohort when compared to controls. On the other hand, when markers of systemic inflammation were compared within the bronchiectasis subgroups, we found evidence for elevated WBC count, CRP and fibrinogen levels in patients with bacterial colonization.
It is known that colonization with pathogenic microorganisms in the airways trigger a cascade of events resulting in local airway inflammation (9,12). A previous study has shown that the inflammation is limited to the airways in patients with bronchiectasis and this inflammation is more intense in colonized patients (9). This inflammation might in turn flood into the systemic circulation and lead to a systemic inflammatory response, as suggested by elevated WBC count, CRP and fibrinogen levels in colonized patients in our study. This finding raises the question of whether systemic inflammation in bronchiectasis during clinically stable period is dependent on bronchiectasis severity, which is closely related to colonization. Wilson et al. showed elevated levels of systemic inflammatory markers (WBC count, ESR and CRP) in bronchiectasis; these inflammatory parameters were significantly correlated with HRCT scores (15). In a study done among patients with diseases that cause end-stage respiratory failure, bronchiectasis patients had higher CRP levels with respect to other diseases that cause respiratory failure (21). CRP levels were also independently associated with mortality in this study (21). In addition, it has been shown that systemic inflammation, as reflected by elevated ESR and CRP levels, is related with rapid decline in FEV1 in patients with bronchiectasis (20). All these data point out to the presence of a systemic inflammatory component in bronchiectasis; this component is probably related to disease severity, and therefore systemic inflammation might only be restricted to severe bronchiectasis cases in whom bacterial colonization is expected. The absence of any significant difference with respect to systemic inflammatory markers between the patient and control groups in our study might be explained by the relatively mild disease severity of our bronchiectasis cohort, as shown by the pulmonary function tests and HRCT findings.
The association between systemic inflammation and disease severity is also supported by the findings observed in the P. aeruginosa group of this study. The most commonly accused microorganism with disease severity and worse clinical outcome in bronchiectasis is P. aeruginosa. The presence of this microorganism during stable period is related with more extensive disease, severe airflow limitation and rapid decline in lung function (20,22,23,24,25). Consistently, in this study, patients with P. aeruginosa colonization had more impairment in pulmonary function tests and more diffuse disease on HRCT. All inflammatory markers in the P. aeruginosa group were higher when compared to other groups; however these differences did not reach statistical significance except for WBC count and fibrinogen levels. We believe that the small number of patients has considerably contributed to the statistical non-significance in this subgroup analysis. Nonetheless, these findings point out to a potential role of colonization with certain microorganisms, particularly P. aeruginosa, in the initiation of low-grade systemic inflammation in bronchiectasis.
We found elevated levels of fibrinogen in colonized patients. The only study in the English literature looking for fibrinogen levels in bronchiectasis reported a significant relationship between fibrinogen levels and patient activity score in St. George Respiratory Questionnaire (26). Other studies, analyzing fibrinogen in respiratory diseases have mostly been performed in COPD patients. High fibrinogen levels were seen both during clinically stable periods and exacerbations of COPD (27). The relationship between fibrinogen and bacterial growth was not evaluated in this study; however elevation of fibrinogen during exacerbations was related with sputum purulence, which might be an indirect sign of bacterial infection. In a previous study performed in clinically stable COPD patients, subjects colonized with potentially pathogenic microorganisms had increased levels of fibrinogen (28). Groenewegen et al. reported elevated fibrinogen level as an independent risk factor for recurrent COPD exacerbations (29). We think that these findings reported for COPD are also valid for bronchiectasis patients and fibrinogen is elevated in bronchiectasis patients with airway colonization.
Although the levels of common systemic inflammatory markers (WBC count, CRP and fibrinogen) were increased in bronchiectasis patients with colonization, we were not able to find a difference in levels of TNF-α and IL-8 between study groups. This finding is similar to the literature, in which serum levels of these cytokines were reported within normal limits, despite elevations in the bronchiectatic airways (9). One previous study has reported elevated plasma TNF-α levels in bronchiectasis patients with severe disease and respiratory failure, supporting the probable relationship between systemic inflammation and disease severity (30).
Some limitations of our study merit consideration. First, the study population was relatively small; we were not able to perform detailed statistical analyses in subgroups stratified for colonization or disease severity. Second, the controls and bronchiectasis patients were not entirely matched; smoking prevalence was unexpectedly higher in the control group (active smoking 40%). This was possibly a reflection of high smoking prevalence in our country (31). Smoking is associated with inflammation and previous studies have shown elevated levels of systemic inflammatory markers, such as WBC count, CRP and fibrinogen, in active smokers (32). This is also true for leptin, which was found to increase in asymptomatic smokers (33). All these data raise the possibility that the high smoking prevalence among controls, might have masked the ongoing systemic inflammation in bronchiectasis patients of our cohort. Third, about half of the patients (52%) in the bronchiectasis group were on inhaled corticosteroid therapy, which potentially might have suppressed the inflammatory response (34). Previous studies have shown that inhaled corticosteroids suppress airway inflammation in bronchiectasis (7). Similarly, Sin et al. showed that inhaled corticosteroid may have systemic effects and can decrease serum CRP levels in COPD patients (35).
In conclusion, bronchiectasis is a disease with definite local inflammation. We were not able to show any evidence for systemic inflammation in the overall bronchiectasis cohort with respect to controls. However, there were findings suggestive of systemic inflammation in patients with colonization. We believe that colonization with pathogenic microorganisms in bronchiectasis might trigger a cascade of events leading to systemic inflammation, which in turn might contribute to disease progression. Further studies are needed to clarify the presence of systemic inflammation in bronchiectasis patients with different degrees of disease severity and colonization.
ACKNOWLEDGEMENT
This study was funded by Hacettepe University Research Foundation.
We would like to thank Alev Oktem, MD for her support in the measurement and assessment of IL-8, TNF-α and leptin levels.
CONFLICT of INTEREST
None declared.
REFERENCES
- Cole PJ. Bronchiectasis. In: Brewis RAL, Corrin B, Geddes DM, Gibson GJ (eds). Respiratory Medicine. 2nd. London: WB Saunders, 1995: 1286-317.
- Fraser RS, Colman N, M?ller NL, Pare PD. Bronchiectasis and other bronchial abnormalities. In: Fraser RS, M?ller NL, Colman N, Pare PD (eds). Fraser and Pare's Diagnosis of Diseases of the Chest. 4th ed. Philadelphia: WB Saunders, 1999: 2265-86.
- Tsang KW, Tipoe GL. Bronchiectasis: not an orphan disease in the East. Int J Tuberc Lung Dis 2004; 8: 691-702. [?zet]
- O'Donnell AE. Bronchiectasis. Chest 2008; 134: 815-23. [?zet] [Tam Metin] [PDF]
- Cole PJ. Inflammation: a two edged-sword- The model of bronchiectasis. Eur J Respir Dis? 1986; 147(Suppl): 6-15. [?zet]
- Barker AF. Bronchiectasis. N Engl J Med 2002; 346: 1383-93.
-
Tsang KW, Ho PL, Lam WK, Ip MS, Chan KN, Ho CS, et al. Inhaled fluticasone reduces
sputum inflammatory indices in severe bronchiectasis. Am J Respir Crit Care Med
1998; 158: 723-7.
[?zet] [Tam Metin] [PDF] - Gaga M, Bentley AM, Humbert M, Barkans J, O'Brien F, Wathen CG, et al. Increases in CD4+ T lymphocytes, macrophages, neutrophils and interleukin 8 positive cells in the airways of patients with bronchiectasis. Thorax 1998; 53: 685-91. [?zet] [PDF]
- Angrill J, Agust? C, De Celis R, Filella X, Ra?? A, Elena M, et al. Bronchial inflammation and colonization in patients with clinically stable bronchiectasis. Am J Respir Crit Care Med 2001; 164: 1628-32. [?zet] [Tam Metin] [PDF]
- Tsang KW, Chan K, Ho P, Zheng L, Ooi GC, Ho JC, et al. Sputum elastase in steady-state bronchiectasis. Chest 2000; 117: 420-6. [?zet] [Tam Metin] [PDF]
- Zheng L, Tipoe G, Lam WK, Ho JC, Shum I, Ooi GC, et al. Endothelin-1 in stable bronchiectasis. Eur Respir J 2000; 16: 146-9. [?zet]
- Fuschillo S, de Felice A, Balzano G. Mucosal inflammation in idiopathic bronchiectasis: cellular and molecular mechanisms. Eur Respir J 2008; 31: 396-406. [?zet]
-
Frieri M. Inflammatory issues in allergic rhinitis and asthma. Allergy Asthma Proc
2005; 26: 163-9.
[?zet] -
Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive
pulmonary disease and systemic inflammation: a systematic review and a
meta-analysis. Thorax 2004; 59: 574-80.
[?zet] [PDF] - Wilson CB, Jones PW, O'Leary CJ, Hansell DM, Dowling RB, Cole PJ, et al. Systemic markers of inflammation in stable bronchiectasis. Eur Respir J 1998; 12: 820-4. [?zet] [PDF]
-
Reiff DB, Wells AU, Carr DH, Cole PJ, Hansell DM. CT findings in bronchiectasis:
limited value in distinguishing between idiopathic and specific types. AJR Am J
Roentgenol 1995; 165: 261-7.
[?zet] [PDF] - Standardized lung function testing: Official Statement of the European Respiratory Society. Eur Respir J Suppl 1993; 16: 1-100.
- Angrill J, Agust? C, de Celis R, Ra?? A, Gonzalez J, Sol? T, et al. Bacterial colonisation in patients with bronchiectasis: microbiological pattern and risk factors.? Thorax 2002; 57: 15-9. [?zet] [PDF]
- Pye A, Stockley RA, Hill SL. Simple method for quantifying viable bacterial numbers in sputum. J Clin Pathol 1995; 48: 719-24. [?zet] [PDF]
- Mart?nez-Garc?a MA, Soler-Catalu?a JJ, Perpi??-Tordera M, Rom?n-S?nchez P, Soriano J. Factors associated with lung function decline in adult patients with stable non-cystic fibrosis bronchiectasis. Chest 2007; 132: 1565-72. [?zet] [Tam Metin] [PDF]
-
Cano NJ, Pichard C, Roth H, Court-Fortun? I, Cynober L, G?rard-Boncompain M, et
al. C-reactive protein and body mass index predict outcome in end-stage
respiratory failure. Chest 2004; 126: 540-6.
[?zet] [Tam Metin] [PDF] - Miszkiel KA, Wells AU, Rubens MB, Cole PJ, Hansell DM. Effects of airway infection by Pseudomonas aeruginosa: a computed tomographic study. Thorax 1997; 52: 260-4. [?zet] [PDF]
- Ho PL, Chan KN, Ip MS, Lam WK, Ho CS, Yuen KY, et al. The effect of Pseudomonas aeruginosa infection on clinical parameters in steady-state bronchiectasis. Chest 1998; 114: 1594-8. [?zet] [PDF]
- Evans SA, Turner SM, Bosch BJ, Hardy CC, Woodhead MA. Lung function in bronchiectasis: the influence of Pseudomonas aeruginosa. Eur Respir J 1996; 9: 1601-4. [?zet]
- Wilson CB, Jones PW, O'Leary CJ, Hansell DM, Cole PJ, Wilson R. Effect of sputum bacteriology on the quality of life of patients with bronchiectasis. Eur Respir J 1997; 10: 1754-60. [?zet] [PDF]
-
Mart?nez-Garc?a MA, Perpi??-Tordera M, Rom?n-S?nchez P, Soler-Catalu?a JJ. Quality-of-life
determinants in patients with clinically stable bronchiectasis. Chest 2005;
128: 739-45.
[?zet] [Tam Metin] [PDF] - Wedzicha JA, Seemungal TA, MacCallum PK, Paul EA, Donaldson GC, Bhowmik A, et al. Acute exacerbations of chronic obstructive pulmonary disease are accompanied by elevations of plasma fibrinogen and serum IL-6 levels. Thromb Haemost 2000; 84: 210-5. [?zet]
- Banerjee D, Khair OA, Honeybourne D. Impact of sputum bacteria on airway inflammation and health status in clinically stable COPD. Eur Respir J 2004; 23: 685-91. [?zet] [Tam Metin] [PDF]
- Groenewegen KH, Postma DS, Hop WC, Wielders PL, Schl?sser NJ, Wouters EF; COSMIC Study Group. Increased systemic inflammation is a risk factor for COPD exacerbations. Chest 2008; 133: 350-7. [?zet] [Tam Metin] [PDF]
- Mart?nez-Garc?a MA, Perpi??-Tordera M, Rom?n-S?nchez P, Soler-Catalu?a JJ, Carratal? A, Yago M, et al. The association between bronchiectasis, systemic inflammation, and tumor necrosis factor alpha. Arch Bronconeumol 2008; 44: 8-14. [?zet]
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2008.
- Yanbaeva DG, Dentener MA, Creutzberg EC, Wesseling G, Wouters EF. Systemic effects of smoking. Chest 2007; 131: 1557-66. [?zet] [Tam Metin] [PDF]
- Vernooy JH, Drummen NE, van Suylen RJ, Cloots RH, M?ller GM, Bracke KR, et al. Enhanced pulmonary leptin expression in patients with severe COPD and asymptomatic smokers. Thorax 2009; 64: 26-32. [?zet]
- Antoniu SA. Effects of inhaled therapy on biomarkers of systemic inflammation in stable chronic obstructive pulmonary disease. Biomarkers 2010; 15: 97-103. [?zet]
-
Sin DD, Lacy P, York E, Man SF. Effects of fluticasone on systemic markers of
inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care
Med 2004; 170: 760-5.
[?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Beg?m Ergan Arsava,
Hacettepe ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
S?hhiye, 06100 ANKARA - TURKEY
e-mail: erganb@hacettepe.edu.tr