Toplum k?kenli Burkholderia cepacia pn?monisi: Ba????kl??? sa?lam iki olgu sunumu
Mehmet BAYRAM1, Mesiha BABALIK2, Nur Dilek BAKAN3, ?sa D?NGEL4
1 SB Sivas Numune E?itim ve Ara?t?rma Hastanesi, G???s Hastal?klar? Klini?i, Sivas,
2 SB Ahi Evren G???s Kalp Damar Cerrahisi E?itim ve Ara?t?rma Hastanesi, Trabzon,
3 SB Yedikule G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi, ?stanbul,
4 SB Sivas Numune E?itim ve Ara?t?rma Hastanesi, G???s Cerrahisi Klini?i, Sivas.
?ZET
Toplum k?kenli Burkholderia cepacia pn?monisi: Ba????kl??? sa?lam iki olgu sunumu
Burkholderia cepacia imm?ns?presif ve yap?sal akci?er hastal??? olan hastalarda k?t? prognozlu pn?moniye neden olan gram-negatif bir basil ailesidir. Bu yaz?da, altta yatan hastal??? olmayan, ba????kl??? sa?lam olan iki hastada t?berk?loz ve malignite ile kar??an B. cepacia pn?monisi sunulmu?tur. Her iki hastada da geni? spektrumlu antibiyotiklere yan?t al?namamas? balgam aside diren?li basil yaymalar?n?n negatif olmas? nedeniyle bronkoskopi uyguland?. Al?nan bron?iyal lavaj ?rneklerinde B. cepacia ?redi. Antibiyogramda her iki hastada da kinolonlara duyarl?l?k saptand?. Kinolon tedavisi ile her iki hastada da klinik ve radyolojik tam d?zelme saptand?. Bu iki hasta sa?l?kl? bireylerde de Burkholderia pn?monisi g?r?lebilece?ini ve tan?da bron? lavaj?n?n ?nemini g?sterdi.
Anahtar Kelimeler: Burkholderia cepacia, bron? lavaj?, kinolon, pn?moni, toplum k?kenli infeksiyonlar.
SUMMARY
Community-acquired Burkholderia cepacia pneumonia: a report of two immunocompetent patients
Mehmet BAYRAM1, Mesiha BABALIK2, Nur Dilek BAKAN3, ?sa D?NGEL4
1 Clinic of Chest Diseases, Sivas Numune Training and Research Hospital, Sivas, Turkey,
2 Ahi Evren Chest Cardiovascular Surgery Training and Research Hospital, Trabzon, Turkey,
3 Yedikule Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey,
4 Clinic of Chest Surgery, Sivas Numune Training and Research Hospital, Sivas, Turkey.
Burkholderia cepacia is a gram-negative bacilli leading to pneumonia with poor prognosis and usually seen in patients with immunsupression or with structural lung diseases. This report is about two patients with no underlying disease diagnosed as B. cepacia pneumonia mimicking malignancy and tuberculosis. Bronchoscopy was applied on both patients since no response to treatment with wide spectrum antibiotics and negative sputum smears for acid-fast bacili. B. cepacia was isolated from bronchial lavage culture. Antibiogram revealed sensitivity to quinolones in both cases. Radiological and clinical complete remission was seen in patients by quinolones. The current cases showed that community-acquired Burkholderia pneumonia is possible in healthy patients. Bronchial washing is important in diagnosis.
Key Words: Burkholderia cepacia, bronchial lavage, quinolone, pneumonia, community-acquired infections.
Burkholderia (previously known as Pseudomonas) cepacia was first described in 1949 by Walter Burkholder, as the phytopathogen responsible for a bacterial rot of onions (1). It was first reported as a human pathogen causing endocarditis in the 1950s (2). B. cepacia is quite widespread in the environment and resistant to many antibiotics and antiseptic solutions (3,4,5). These agents are factors of potentially fatal pneumonia in patients with suppressed immunity, especially cystic fibrosis or chronic granulomatous disease (6). B. cepacia is also reported to cause epidemics of nosocomial respiratory infections through contamination of medical devices (7,8).
It has been shown that the organism have antifungal and degradative properties which have created interest in its potential use as a biological control agent to improve crop yields and its use for the bioremediation of contaminated soils (9). In contrast to its potential agricultural benefits, B. cepacia has also emerged as a multiresistant opportunist human pathogen, leading to concern about the relationship between environmental and clinical isolates and the potential hazards of releasing B. cepacia as a biological control agent (9). This report is about two patients with no underlying disease diagnosed as community-acquired B. cepacia pneumonia mimicking malignancy and tuberculosis, which resolved completely with quinolone treatment.
CASE REPORT
Case 1, a 60-year-old male was evaluated with malaise and productive cough lasting for 10 days. Case 2, 66-year-old male was admitted because of a 5-days history of cough and expectoration of purulent sputum. The patients had a smoking history of 30 and 25 packs-year, respectively. Both had previously been healthy and reported no history of hospitalization for the last year. They declared no family history of any pulmonary illness or chronic disease like diabetes mellitus. Case 1 has been worked as a servant in an office and got retired 6 years ago. Case 2 was formerly a farmer but has not been worked for approximately ten years.
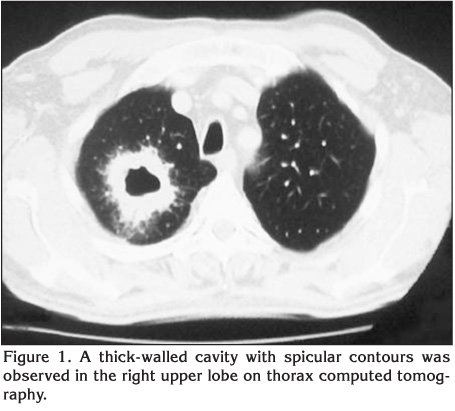
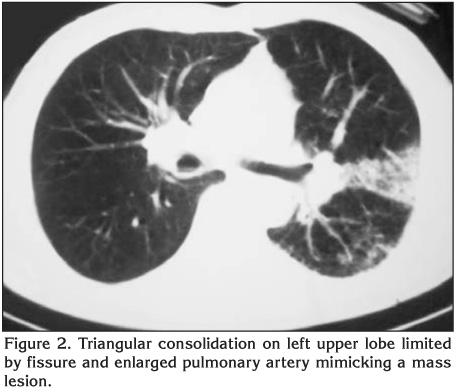
Their physical examinations were normal, as were the oxygen saturations. Laboratory studies showed on admission a total WBC count of 13.100/mm3 and 7.200 mm3, an erythrocyte sedimentation rate of 96 mm/hour and 90 mm/hour, a C-reactive protein of 174 mg/dL and 8.85 mg/dL for Case 1 and Case 2, respectively. Both had normal levels of glucose and electrolytes, and normal renal and hepatic function tests. Case 1 had an irregular cavitary lesion, about 3 cm in diameter, with air-fluid level in the upper zone of right hemithorax on chest X-ray. Chest X-ray of case 2 revealed heterogeneous density on left lower zone. Both had negative sputum smears for acid-fast bacilli (AFB). Gram-positive diplococci were seen on sputum Gram-stain of case 1 and abundance of PNL and gram-positive cocci of case 2. No growth was detected on both sputum cultures. Case 1 was started on ceftriaxone 2 g/day intravenous (IV) and clarithromycin 1 g/day PO, case 2 was started on ampicillin/sulbactam 4 g/day IV and clarithromycin 1 g/day PO. A thorax computed tomography (CT) was performed when no improvement was achieved with empiric antibiotherapy. A thick-walled cavity with spicular contours was observed on thorax CT of case 1 (Figure 1). Case 2 had a triangular consolidation in the lingular segment of the left upper lobe on CT (Figure 2). Fiberoptic bronchoscopy was performed to case 1 with a suspicion of bronchial carcinoma and to case 2 with a suspicion of obstructive pneumonia. Both had no endobronchial pathology and no malignant cells were detected on cytological examination of their bronchial lavage and post-bronchoscopic sputums. Lavage and post-bronchoscopic sputum smear results were negative for AFB. B. cepacia grew on bronchial lavage cultures of the cases. Antibiogram was reported to be resistant to amoxicillin/clavulanic acid, ticarcillin, ceftriaxone, cefuroxime, ureidopen, cefoxitin, and co-trimoxazole while sensitive to ceftazidime, imipenem, amikacin, gentamicin, ciprofloxacin, piperacillin/tazobactam, meropenem and less sensitive to cefepime in Case 1 and it was reported to be resistant to gentamicin, imipenem, amikacin, aztreonam, cefepime, and piperacillin whereas sensitive to ceftazidime, ciprofloxacin, and levofloxacin in Case 2. Case 1 received ciprofloxacin 750 mg PO bid and case 2 levofloxacin 500 mg/day IV significant radiological improvement was observed (Figure 3). Final laboratory findings were; WBC count 7200/mm3 and 6040 mm3, erythrocyte sedimentation rate 12 mm/hour and 34 mm/hour, and C-reactive protein 2.6 mg/dL and 0.4 mg/dL for Case 1 and Case 2, respectively. All sputum and bronchial lavage cultures of the patients remained negative for Mycobacterium tuberculosis. Both patients are currently under follow-up and have no complaint.

DISCUSSION
B. cepacia complex is a family of catalase-producing, non-lactose-fermenting gram-negative bacteria comprising 9 sub-groups. They cause pneumonia in immunocompromised persons, particularly in those with cystic fibrosis and chronic granulomatous disease. It is rarely encountered in individuals with a normal immune system and without a structural lung disease. To date, community-acquired pneumonia caused by B. cepacia has been reported in a small number of individuals without an underlying disease. Firstly Waterer et al. described a community-acquired pneumonia caused by B. cepacia in healthy adult (10). In present study, absence of hospitalization eliminates the possibility of nosocomial infection in both cases. Microbiology laboratory records were examined in terms of probability of laboratory contamination and it was seen that B. cepacia was not produced on any material before. Since case 1 was presented with a cavitary lesion in the right upper zone, tuberculosis was considered as diagnosis in the first place. Due to negative sputum smears for AFB, thick cavity wall along with his smoking history and advanced age, malignity was also strongly considered. The triangular consolidation of lingular segment and a suspicious central mass appearance as well as the patient's smoking history and advanced age of case 2 suggested also malignity. The noteworthy aspects of both cases include the fact that they are not immunocompromised patients, absence of chronic lung disease as well as no chronic lung disease patients in their close circles, and lack of the possibility of nosocomial infection due to absence of hospitalization.
Bacterial culture of bronchoscopic lavage has been the method of diagnosis in both cases. Demir et al. have reported a hemodialysis patient with cavitary lesion in the right lung upper zone, similar to case 1 (11). B. cepacia was isolated from his bronchial lavage culture too and he recovered also after ciprofloxacin treatment. To note, he was a diabetic hemodialysis patient and had a central catheter. Cultivation of bronchial lavage seems to be important in the diagnosis of B. cepacia pneumonia.
Because of its inherent resistance to many antibiotics the organism can be difficult to treat. Both strains of the current cases were sensitive to quinolones and the antibiotherapy resulted with complete resolution. Waterer and Demir also treated successfully their patients with quinolone antibiotics (10,11). The unusual susceptibility to antibiotics suggested that it is not transmitted from someone with chronic lung disease. The anti-tuberculous effects of quinolones, could naturally raise a suspicion of possibility of tuberculosis. However, cultures of all specimens remained negative for M. tuberculosis.
It has been shown that the organism have remarkable potential as an agent for both biodegradation and biocontrol, thus it is being considered as a plant-growth-promoting rhizobacterium (9). Used as a pesticide and biofertilizer in agriculture, that B. cepacia can be transmitted to humans via contaminated products is generally accepted. Its development in out-of-hospital settings and immunocompetent cases may possibly be attributed to environmental exposure. But we were not able to confirm the use for this purpose in our country.
These two cases have demonstrated that B. cepacia, which was previously considered as merely an opportunistic infection factor, may be encountered in individuals that are not in the risk group. Could this also be a sign of we would be likely to encounter this difficult and variable organism as a community-acquired pneumonia agent more frequently in the future?
CONFLICT of INTEREST
None declared.
REFERENCES
- Burkholder W. Sour skin, a bacterial rot of onion bulbs. Phytopathology 1950; 40: 115-8.
- Holmes A, Govan J, Goldstein R. Agricultural use of Burkholderia (Pseudomonas) cepacia: a threat to human health? Emerg Infect Dis 1998; 4: 221-7. [?zet] [PDF]
- Hancock RE. Resistance mechanisms in Pseudomonas aeruginosa and other nonfermentative gram-negative bacteria. Clin Infect Dis 1998; 27: 93-9. [?zet] [PDF]
- Mortensen JE, Fisher MC, LiPuma JJ. Recovery of Pseudomonas cepacia and other Pseudomonas species from the environment. Infect Control Hosp Epidemiol 1995; 16: 30-2. [?zet]
- Oie S, Kamiya A. Microbial contamination of antiseptics and disinfectants. Am J Infect Control 1996; 24: 389-95. [?zet]
- Muhdi K, Edenborough FP, Gumery L, O'Hickey S, Smith EG, Smith DL, et al. Outcome for patients colonised with Burkholderia cepacia in a Birmingham adult cystic fibrosis clinic and the end of an epidemic. Thorax 1996; 51: 374-7. [?zet] [PDF]
- Takigawa K, Fujita J, Negayama K, Yamagishi Y, Yamaji Y, Ouchi K, et al. Nosocomial outbreak of Pseudomonas cepacia respiratory infection in immunocompromised patients associated with contaminated nebulizer devices. Kansenshogaku Zasshi 1993; 67: 1115-25. [?zet]
- Loukil C, Saizou C, Doit C, Bidet P, Mariani-Kurkdjian P, Aujard Y, et al. Epidemiologic investigation of Burkholderia cepacia acquisition in two pediatric intensive care units. Infect Control Hosp Epidemiol 2003; 24: 707-10. [?zet]
- Govan JRW, Hughes JE, Vandamme P. Burkholderia cepacia: medical, taxonomic and ecological issues. J Med Microbiol 1996; 45: 395-407. [?zet] [PDF]
- Waterer GW, Jones CB, Wunderink RB. Bacteremic community-acquired pneumonia in an immunocompetent adult due to Burkholderia cepacia. Chest 1999; 116: 1842-3. [Tam Metin] [PDF]
- Demir S, Fidan F, De?irmenci B, ?zer Y,? G?k?e ?.? Burkholderia cepacia pneumonia mimicking invasive aspergillosis in a hemodialysis patient. Toraks 2005; 6: 175-7. [?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Mehmet BAYRAM,
SB Sivas Numune E?itim ve
Ara?t?rma Hastanesi,
G???s Hastal?klar? Klini?i,
S?VAS - TURKEY
e-mail: drmehmetbayram@yahoo.com