Actinomyces israelii: Torasik ampiyemin nadir bir nedeni
Athanassios
KleontaS1, Christos Asteriou1, Andreas Efstathiou1, Eleftheria Konstantinou2,
Charilaos Tsapas2, Nikolaos Barbetakis1
1 Theagenio Hastanesi, G???s Cerrahisi B?l?m?, Thessaloniki, Yunanistan,
2 Theagenio Hastanesi, Solunum Hastal?klar? B?l?m?, Thessaloniki, Yunanistan.
?ZET
Actinomyces israelii: Torasik ampiyemin nadir bir nedeni
Actinomyces israelii genellikle kronik s?p?ratif ve gran?lomat?z infeksiyonlara neden olur. Aktinomikoza ba?l? izole plevral ef?zyon nadirdir. Burada, A. israelii'nin neden oldu?u, ani ba?layan, h?zla bozulan ve g???s t?p drenaj? ve antibiyoterapiye yan?t vermeyen nadir bir torasik ampiyemli olgu sunulmaktad?r. Sol posterolateral torakotomi ile ampiyem drenaj? ve viseral pariyetal pl?rektomi ile tedavi edildi ve kal?c? ??z?m sa?land?.
Anahtar Kelimeler: Torasik ampiyem, cerrahi.
SUMMARY
Actinomyces israelii: a rare cause of thoracic empyema
Athanassios
KleontaS1, Christos Asteriou1, Andreas Efstathiou1, Eleftheria Konstantinou2,
Charilaos Tsapas2, Nikolaos Barbetakis1
1 Department of Chest Surgery, Theagenio Hospital, Thessaloniki, Greece,
2 Department of Respiratory Medicine, Theagenio Hospital, Thessaloniki, Greece.
Actinomyces israelii usually causes chronic suppurative and granulomatous infections. Isolated pleural effusion due to Actinomycosis is rare. This report describes an unusual case of thoracic empyema caused by A. israelii with sudden onset and rapid deterioration that failed to respond to chest tube drainage and antibiotherapy. Empyema drainage and visceral parietal pleurectomy by a left postolateral thoracotomy proved to be of vital importance and a permanent solution.
Key Words: Empyema thoracic, surgery.
Thoracic actinomycosis is a relatively uncommon anaerobic infection and thoracic empyema caused by Actinomyces israelii is very rare (1). The diagnosis of actinomycosis requires a high degree of clinical suspicion. A case of an acute thoracic empyema threatening a patient's life is presented. Surgical intervention literally saved patient's life, since conservative treatment with chest tube drainage and antibiotics failed to stabilize her clinical condition. A. israelii as the reason of the empyema was revealed later by the cultures. To the best of our knowledge, there is limited number of similar cases announced in the English literature.
Case REPORT
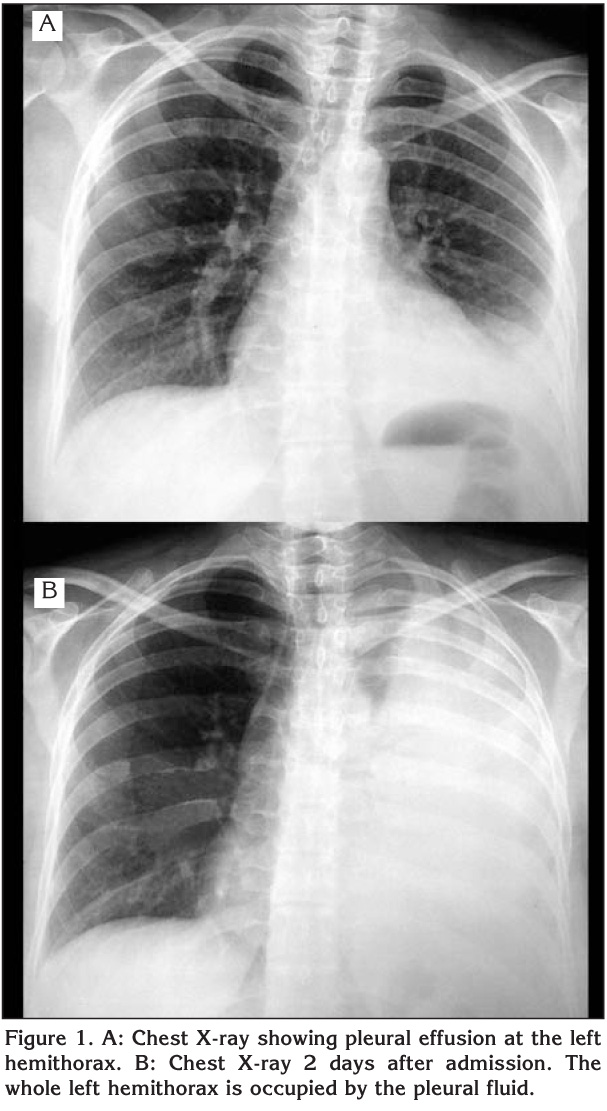
A 35-year-old woman was admitted to our hospital due to an acute left chest pain, extending to the sternum, accompanied by shortness of breath. Her pulse rate was 115/min combined with blood pressure of 105/60 mmHg. The respiratory rate was 25/min, oxygen saturation 89-91% and the axilla temperature was measured 38.8?C. Physical examination revealed reduced respiratory whispering at the left basis. Chest X-ray showed pleural effusion on the left, while the needle thoracentesis performed, attributed clear, yellowish liquid (Figure 1A). Two days later, a new chest X-ray indicated rapid deterioration and the performed chest computed tomography scan revealed extensive pleural effusion on the left (Figure 1B, Figure 2A). A chest tube was inserted and 2.300 mL of clear, yellowish liquid were drained. Six days later, a new chest computed tomography scan showed encapsulated collection at the top of the left lung, while the fever insisted with axilla temperature climbing at 39.2?C (Figure 2B).

Due to these findings, the patient underwent a left posterolateral thoracotomy and an empyema was brought to light. Empyema drainage in combination with visceral and parietal pleurectomy was performed. Drainage of pus from the chest tube continued for two weeks thereafter. Gram stains of the empyema fluid revealed gram-positive organisms characterized by suppuration, sinus tract formation and purulent discharge containing yellowish "sulfur granules". Aerobic and anaerobic cultures of the empyema fluid grew only A. israelii. Intravenous ampicillin, 1 g twice/day, was the antibiotherapy of choice.
Within 48 hours her condition improved and her temperature returned to normal. Intravenous ampicillin was continued at the higher dose for 10 days and followed by one week of oral ampicillin, 2 g daily. The patient was discharged without any medication on the 18th postoperative day. Six weeks after admission her radiograph is clear, while she is asymptomatic (Figure 3).

Discussion
The genus Actinomyces consists of gram-positive anaerobic organisms. Actinomycosis is a chronic, suppurative granulomatous infection. It typically involves cervicofacial and abdominopelvic organs. Thoracic involvement is much less frequent. Actinomyces species are commensals of the human oropharynx, gastrointestinal tract and female genitalia. Infection is established first by a breach of the mucosal barrier during various procedures (dental, gastrointestinal), aspiration or pathologies such as diverticulitis (2).
Thoracic actinomycosis is very rare. It is often misdiagnosed as a neoplasm, as it forms a mass that extends to the chest wall. It is characterized by suppuration, sinus tract formation, and purulent discharge containing yellowish "sulfur granules" (3). It arises from aspiration of organisms from the oropharynx, which may cause atelectasis and pneumonitis. The initial acute inflammation is followed by the chronic and indolent phase of the disease that generates abscesses, necrosis, and fibrosis of lung parenchyma, which commonly cavitates. It progresses slowly without respecting anatomic boundaries, such as interlobar fissures or the chest wall. If not recognized, the parenchymal disease invades the pleura, the chest wall, soft tissues, and bony structures (4). The clinical symptoms of thoracic actinomycosis frequently include fever, chills, hemoptysis, cough, pleuritic chest pain, and anemia. It may be presented as thoracic empyema, superior vena cava syndrome or pericardial effusion in advanced disease (5).
The treatment of actinomycosis includes antimicrobial therapy with or without surgery. Penicillin is the antibiotic of choice, although other antimicrobial agents, such as clindamycin, tetracycline or erythromycin, can be used in cases of penicillin allergy. The optimal duration of antimicrobial therapy should be tailored depending on the severity of illness. However, a longer duration of treatment with antimicrobial agents is usually necessary, since the premature termination of antimicrobial therapy may cause a relapse of actinomycosis. When there is an empyema, in order to prevent the spread of the disease, surgical intervention still remains the curative option (6).
In conclusion, the diagnosis of actinomycosis related to the acute thoracic empyema requires a high index of clinical suspicion because it is very rare. In addition, when conservative treatment is not effective, it is essential not to delay to perform an emergency thoracotomy and drain empyema.
CONFLICT of INTEREST
None declared.
REFERENCES
- Lu MS, Liu HP, Yeh CH, Wu YC, Liu YH, Hsieh MJ, et al. The role of surgery in hemoptysis caused by thoracic actinomycosis; a forgotten disease. Eur J Cardiothorac Surg 2003; 24: 694-8. [?zet]
- Smego R, Foglia G. Actinomycosis. Clin Infect Dis 1998; 26: 1255-63. [PDF]
- Touboul JL, Chaussade F, Desvignes B, Mangeney T, Bidault C. Isolated pleural actinomycosis. A propos of 2 cases. Rev Pneumol Clin 1990; 46: 69-72. [?zet]
- Spinola SM, Bell A, Henderson FW. Actinomycosis: a case of pulmonary and mediastinal mass lesions in children. Am J Dis Child 1981; 135: 336-9. [?zet]
- Chao D, Nanda A. Spinal epidural abscess: a diagnostic challenge. Am Fam Physician 2002; 65: 1341-6. [?zet]
- Honda H, Bankowski MJ, Kajioka EH, Chokrungvaranon N, Kim W, Gallacher ST. Thoracic vertebral actinomycosis: Actinomyces israelii and Fusobacterium nucleatum. J Clin Microbiol 2008; 46: 2009-14. [?zet] [Tam Metin] [PDF]
Yaz??ma Adresi (Address for Correspondence):
Dr. Nikolaos Barbetakis,
A. Simeonidi 2
THESSALONIKI - GREECE
e-mail: nibarbet@yahoo.gr