Bronkojenik kist i?in nadir bir sunum: Presternal, subk?tan?z ve 42 ya??nda erkek
Timu?in ALAR1, Asl? MURATLI2
1 ?anakkale Onsekiz Mart ?niversitesi T?p Fak?ltesi, G???s Cerrahisi Anabilim Dal?, ?anakkale,
2 ?anakkale Onsekiz Mart ?niversitesi T?p Fak?ltesi, Patoloji Anabilim Dal?, ?anakkale.
?ZET
Bronkojenik kist i?in nadir bir sunum: Presternal, subk?tan?z ve 42 ya??nda erkek
Bronkojenik kistler genellikle do?umdan hemen sonra veya erken ?ocukluk d?neminde saptan?r. Lezyonlar?n b?y?k ?o?unlu?u mediasten, trakeobron?iyal a?a? boyunca veya akci?er parankiminde bulunur. K?tan?z veya subk?tan?z bronkojenik kistler nadir rapor edilmi?tir. Olgumuz ?ngilizce literat?rde eri?kin ya?taki manubrium sterni ?zerinde kist saptanan ikinci hastad?r. Cerrahi total eksizyon kesin tedavi y?ntemi olup, ince i?ne aspirasyonu mukoepidermoid karsinom ve malign melanoma geli?ti?i bildirildi?inden denenmemelidir.
Anahtar Kelimeler: Bronkojenik kist, presternal, subk?tan?z.
SUMMARY
A rare presentation of a bronchogenic cyst: presternal, subcutaneous and 42-year-old man
Timu?in ALAR1, Asl? MURATLI2
1 Department of Chest Surgery, Faculty of Medicine, Canakkale Onsekiz Mart University, Canakkale, Turkey,
2 Department of Pathology, Faculty of Medicine, Canakkale Onsekiz Mart University, Canakkale, Turkey.
Bronchogenic cysts are generally detected shortly after birth or in early childhood. Most lesions are found in the mediastinum, along the tracheobronchial tree or in the lung parenchyma. Cutaneous or subcutaneous bronchogenic cysts are rarely reported. Our patient was the second case in the English literature who had a cyst over the manubrium sterni in adult life. Surgical total excision is the definitive treatment of extrathoracic bronchogenic cysts, needle aspiration management should not be tried because of association with malignant lesions as mucoepidermoid carcinoma and malign melanoma have been reported to arise from them.
Key Words: Bronchogenic cyst, presternal, subcutaneous cyst.
Geli? Tarihi/Received: 16/06/2011 - Kabul Edili? Tarihi/Accepted: 20/09/2011
Bronchogenic cysts are generally detected shortly after birth or in early childhood. These lesions are benign congenital developmental anomalies of the tracheobronchial buds from the primitive foregut (1). Most lesions are found in the mediastinum, along the tracheobronchial tree or in the lung parenchyma (2). Cutaneous or subcutaneous bronchogenic cysts are rarely reported. The most common location of these lesions are suprasternal notch, presternal area, neck and scapula (3). During embryogenesis, bronchial buds may be pinched off the developing lung by midline fusion of sternal bars. The resulting presternal bronchogenic cyst usually becomes apparent in early childhood, have occured rarely in adults life and we were able to find one case reported in the English literature (4).
CASE REPORT
A 42-year-old man, heavy smoker (25 packet/year) was referred to our clinic after resection of subcutaneous, painless, 3 cm in diameter, non-tender, soft and mobile mass lesion at the manubrium sterni (Figure 1). Histopathologic examination was reported a bronchogenic cyst.

The mass on the manubrium sterni had been present since birth that progressed in size with age. The patient did not complain about any respiratory disturbance or swallowing difficulty. On physical examination, a 3 cm incision scar tissue over the manubrium sterni and left inguinal scar tissue (varicocele operation in 1996) was noted. His chest radiograph and laboratory investigations were within normal limits. A contrast-enhanced computed tomography (CT) scan of the neck and chest demonstred bilateral emphysemateous areas in the lung and 16 mm hypodens lesion in the right lob of the thyroid gland. Fine needle aspiration biopsy of this nodule reported as benign cytology.
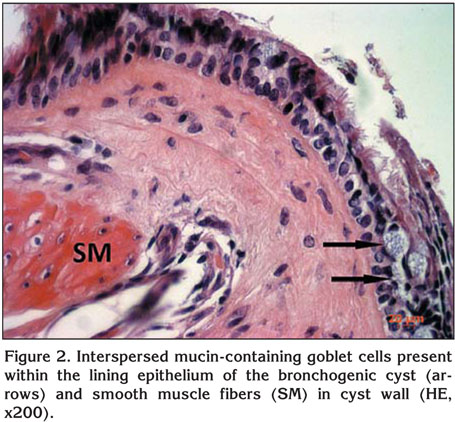
Paraffin blocks of cyst were wanted and observed again. Pathologic examination demonstrated a cystic structure lined by ciliated pseudostratified columnar epithelium with scattered mucin-containing goblet cells. The cyst wall was composed of fibrocollagenous tissue and smooth muscle fibers (Figure 2).
DISCUSSION
Bronchogenic cysts are rare and congenital anomalies that are typically located in the mediastinum or lung parenchyma (5). An abnormal budding of the tracheobronchial system between the 22nd and 33rd days of gestation and persistence of such a bud may give rise to bronchogenic cyst. Abnormal migration of a bud may occur during the course of development and rest in different intrathoracic or extrathoracic locations (6). In the literature, more than 80 cutaneous or subcutaneous bronchogenic cysts have been reported and most are diagnosed in early childhood with 2 cases reported after the age of 18 like our patient (7). Our patient was the second case in the English literature who had a cyst over the manubrium sterni in adult life.
Bronchogenic cysts occur primarily in males in a ratio of approximately 4:1 and are present at birth (7,8). Larger cysts may cause pressure symptoms like dyspnea, respiratory distress, cough and dysphagia. Rarely, they may present as a fistulous opening or an abscess and hoarseness (6,9).
A definitive diagnosis of bronchogenic cysts requires histopathological confirmation. Bronchogenic cysts are lined by a mucosa consisting of pseudostratified columnar epithelium. Some of the epithelial cells show cilia extending into the lumen. Goblet cells may be interspersed. The wall frequently contains smooth muscle and mucous glands but only rarely contains cartilage (10). Our diagnosis was confirmed with the demonstration of ciliated pseudostratified columnar epithelium admixed with goblet cells and smooth muscle fibers.
The differential diagnosis of bronchogenic cysts may include; cutaneous ciliated cyst, epidermal inclusion cyst, thyroglossal duct cyst, trichilemmal cyst, branchial cyst and dermoid cyst (1,10,11). Cysts of a branchial or thyroglossal origin may contain respiratory epithelium, but smooth muscle fibers, cartilages or mucous glands should be absent. Cutaneous ciliated cysts are found very rarely in females as a single lesion, largely on the lower extremities. These cysts show numerous papillary projections lined by a simple cuboidal or columnar ciliated epithelium that resemble fallopian tubes. Mucin-secreting cells are absent. Dermoid cysts are lined by an epidermis that possesses various epidermal appendages that are usually mature. Epidermal inclusion cysts are lined by stratified squamous epithelium. The lining of trichilemmal cysts are composed of squamous epithelium without granular cell layer.
Surgical total excision is the definitive treatment of extrathoracic bronchogenic cysts, needle aspiration management should not be tried because of association with malignant lesions as mucoepidermoid carcinoma and malign melanoma have been reported to arise from them (12,13).
CONFLICT of INTEREST
None declared.
REFERENCES
- Park HS, Son HJ, Kang MJ. Cutaneous bronchogenic cyst over the sternum. The Korean Journal of Pathology 2004; 38: 333-6.
- Lorenzo MD, Collin PP, Vaillancourt R, Duranceau A. Bronchogenic cyst. J Pediatr Surg 1989; 10: 988-91. [?zet]
- Zvulunov A, Amichai B, Grunwald MH, Avinoach I, Halevy S. Cutaneous bronchogenic cyst: delineation of a poorly recognized lesion. Pediatr Dermatol 1998; 15: 277-81. [?zet]
- Hameed SM, Chan WK, Neuman GD, Urschel JD. Presternal bronchogenic cyst in an adult. Plast Reconstr Surg 1993; 92: 763-4.
- Haller JA, Shermeta DW, Donahoo JS, White JJ. Lifethreatening respiratory distress from mediastinal mass in infants. Ann Thorac Surg 1975; 19: 365-70. [?zet]
- Gaikwad P, Muthusami JC, Raj JP, Rajinikanth J, John GM. Subcutaneous bronchogenic cyst. Otolaryngol Head Neck Surg 2006; 135: 951-2.
- Shah SK, Stayer SE, Hicks MJ, Brandt ML. Suprasternal bronchogenic cyst. J Pediatr Surg 2008; 43: 2115-7. [?zet]
- Ustundag E, Iseri M, Keskin G, Yayla B, Muezzinoglu B. Cervical bronchogenic cysts in head and neck region. J Laryngol Otol 2005; 119: 419-23. [?zet]
- Ergin M, Ye?insu A, ?elik A, Onuk Filiz N. A case of cervical bronchogenic cyst presenting with hoarseness in an adult. T?berk?loz ve Toraks Dergisi 2009; 57: 73-6. [?zet] [PDF]
- Kirkham N. Tumors and cysts of the epidermis. In: Elder D (ed). Lever's Histopathology of The Skin. 8th ed. Philadelphia: Lippincott & Raven, 1997: 685-746.
- Ramon R, Betlloch I, Guijarro J, Banuls J, Alfonso R, Silvestre JF. Bronchogenic cyst presenting as a nodular lesion. Pediatr Dermatol 1999; 16: 285-7. [?zet]
- Tanaka M, Shimokawa R, Matsubara O, Aoki N, Kamiyama R, Kasuga T, et al. Mucoepidermoid carcinoma of the thymic region. Acta Pathol Jpn 1982; 32: 703-12. [?zet]
- Tanita M, Kikuchi-Numagami K, Ogoshi K, Suzuki T, Tabata N, Kudoh K, et al. Malignant melanoma arising from cutaneous bronchogenic cyst of the scapular area. J Am Acad Dermatol 2002; 46 (2 Suppl): S19-S21. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Timu?in ALAR,
?anakkale Onsekiz Mart ?niversitesi T?p Fak?ltesi,
G???s Cerrahisi Anabilim Dal?,
17100 ?ANAKKALE - TURKEY
e-mail: timalar@comu.edu.tr