Ya?l?larda ast?m tan?s? farkl? m?d?r?
Arzu YORGANCIO?LU, Ay??n ?AKAR CO?KUN
Celal Bayar ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, Manisa.
?ZET
Ya?l?larda ast?m tan?s? farkl? m?d?r?
Ya?l? pop?lasyonda ast?m yetersiz tan? ve tedavi almaktad?r, ancak bu ya? grubunda mortalite olduk?a y?ksektir. Ya?lanmaya ba?l? akci?erlerde geli?en fizyolojik de?i?iklikler, komorbid durumlar ve ila? kullan?mlar? tipik ast?m tablosunu ya?l?larda de?i?tirebilmekte ve tan?da zorluk yaratmaktad?r. Bu nedenle ba?ta kronik obstr?ktif akci?er hastal??? olmak ?zere t?m ay?r?c? durumlar? g?z ?n?ne alarak do?ru tan? konulmal?d?r, ??nk? do?ru hasta y?netimi hastal?k morbidite ve mortalitesini de?i?tirecektir.
Anahtar Kelimeler: Ast?m, ya?l?larda ast?m, tan? zorlu?u.
SUMMARY
Is the diagnosis of asthma different in elderly?
Arzu YORGANCIO?LU, Ay??n ?AKAR CO?KUN
Department of Chest Diseases, Faculty of Medicine, Celal Bayar University, Manisa, Turkey.
Asthma is mis-diagnosed, under-diagnosed and under-treated in older populations but has a high mortality rate. The physiological changes due to aging of lung, the co-morbid situations and poly pharmacy may change the typical presentation of asthma in older people and cause diagnostic difficulties. But it therefore should be diagnosed properly by taking of all differential situations especially chronic obstructive pulmonary disease into consideration since the appropriate management of the disease will alter the morbidity and mortality.
Key Words: Asthma, asthma in elderly, diagnostic difficulties.
Geli? Tarihi/Received: 01/07/2011 - Kabul Edili? Tarihi/Accepted: 03/07/2011
Elderly population [according to the criteria of World Health Organization (WHO), the population aged 65 and above] is the most increasing age range because of the lifetime gets longer in the developed countries. According to data from WHO data, this group of 600.000 people in 2000 is predicted to increase to 1.2 billion people in 2025. Of these persons, 80-85% have chronic diseases. As all the world, the majority of non-infectious chronic diseases gain importance in this age group.
Diagnosis of asthma that is one of the often seen chronic pulmonary diseases in this group, differs compared to the other age groups and is not easy to be established due to the age related physiological changes. Therefore, its diagnosis and treatment are often less (1,2,3).
In this article the situations, those are different in the elderly asthma will be discussed and the requirements from an accurate diagnosis will be reviewed.
Physiological Changes in the Aging Lungs
Capacity of the aging lung physiologically reduces by 40% or more even in the healthy individuals.
These physiological changes are the extension of the air spaces without alveolar destruction, reduction in the gas exchange surface and loss of the supportive tissue in the peripheral air ways. As a result of these changes, static elastic recoil decreases, residual volume (RV) and Functional Residual Capacity (FRC) increase. Compliance of the chest wall declines and the respiratory work increases.
As the people get older, respiratory muscle strength decreases, and this is directly related to the person's nutritional status. Decrease of the expiratory flow leads to a change in the flow volume curve similar to the small airway obstruction.
Imbalance of the ventilation/perfusion increases due to early closure of the distal air ways. Strength and efficiency of the coughing decrease. Hypoxia sensitivity of the respiratory centers decreases and the response to the airway obstruction may change.
Bronchial hyperreactivity (BHR) increases, but a disturbance occurs in the perception of bronchoconstriction (perception defect). Reduction in the sensitivity of the lung receptors is also effective in this perception defect. Awareness of the shortness of breath is less in this group due to the perception defect and this causes to delay and mistakes in the diagnosis. These aging related changes can mimic the obstructive pulmonary diseases (4).
Epidemiology of Asthma in the Elderly
Prevalence of asthma is same with the other age groups by 6.5-17% (15%), but the diagnosis rate is quite low (1,3). Therefore, the prevalence is considered to be higher than these values.
Mortality rate is much higher than the other age groups. Majority of the persons died from asthma are aged 65 and above. Death rate is 2.8/100.000 between 55-59 years old, while it increases to 4.2/100.000 between 60 and 64 (2,5).
Risk Factors
Atopy is less compared to the young asthmatics, but higher than the controls in the same age group. History of allergy is reported by 29% and skin test positivity by 35%. Sensitivity to the household allergens, particularly to the house dust mite is higher. Outdoor allergens are less with most frequently grass pollen in Europe and ragweed in the USA (3,4,6). Of those persons with rhinitis, 50% have persistent mediate to severe rhinitis.
Diagnostic Difficulties
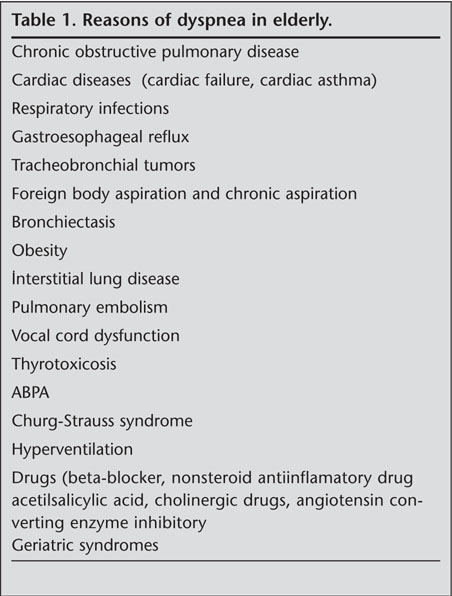
Presentation to a physician or hospital is less in this age group because of the social isolation is more. However, besides this social phenomenon, aging related physiological changes described above making the diagnosis difficult, and can mimic the obstructive pulmonary diseases. There is shortness of breath in one out of every 3 persons in the aged 70 age above group, but it may be caused by any reason described in Table 1.
Differential diagnosis is important for these diseases, but another complicating condition is concomitant asthma. Comorbidity is often seen in this age group and may alter the classical asthma symptoms. Frequent association with systemic inflammatory and metabolic diseases such as ASVD (arteriosclerotic vascular disease), vascular disorders, diabetes mellitus and obesity was seen in asthma, which is also a systemic inflammatory disease (1).
The symptoms due to deterioration of the cognitive functions and perception defects are not typical as we used to see in asthma, and their physical examination is considerably nonspecific (2,3).
Three situations should be considered when evaluating the obstructive diseases in elderly patients:
1. Aged asthmatics with young onset,
2. Asthmatics emergent over 65 years old (Late onset),
3. Chronic obstructive pulmonary disease (COPD).
Basic characteristics of these situations are described in Table 2 (1,5).

Meanwhile, the form of intrinsic asthma which is seen in the elderly should be kept in mind. Intrinsic asthma may be seen in each age group. This is not atopic and often the viral infections are the triggers. The pathogenesis differs from the extrinsic asthma, and intrinsic asthma is often precipitated by an upper respiratory tract infection (3,7,8). It is more common in females and has a higher sensitivity to the sinusitis, nasal polyps and aspirin, and is resistant to the treatment.
As it is seen in the table, clinical features of the early onset asthmatics are more similar to COPD, while the respiratory functions of the late onset asthmatics are more similar to COPD. Because the permanent structural changes are seen more in this group and thus, differential diagnosis with COPD is more difficult due to process to the chronic obstruction. Whereas the permanent structural changes and functional loss are seen less in the late onset asthma because of the reversibility is more and the duration for remodeling is less. However, reduction in the diffusion capacity and the radiological findings are seen less in both early and late onset asthmatics compared to COPD (5,9).
As it is known, air way inflammation is different in COPD and asthma. However, the inflammation has been considered to present similarity with COPD following the development of the fixed air way obstruction in the asthmatics, and numerous studies have been conducted about the inflammation on this subject. Eosinophilic inflammation has been shown to differ still between the groups of the same age and the same levels of the obstruction and reversibility. Although fixed Air way obstruction is developed in the asthmatic, characteristic of the inflammation does not change and differs from the COPD, and eosinophilic inflammation progresses more obviously than in those with COPD. This is why the prognosis of the diseases and response to the steroids are better in the asthmatics.
Asthma and COPD differentiation should be definitely done even the fixed air way obstruction has developed. Therefore, evaluation of the inflammation is important for all the obstructive patients with the same situation (2,10,11,12,13).
By this way, proper approach/plan (e.g. avoiding from the allergens, smoking cessation) for the disease can be done, treatment approach and expectations will differ in both diseases, particularly in terms of the inhaled corticosteroids and cost/efficiency loss may develop due to improper treatments will be reduced, more appropriate treatment of the concomitant diseases (difference of the beta blockers used in both disease) can be done and consequently there will be a difference between the morbidity (annual FEV1 loss 70 mL/5 mL), 10-year mortality (60%/15%) and prognosis in COPD/asthma (2,14).
However, the severe asthmatics with fixed air way obstruction those present neutrophilic inflammations and don't give a response to the reversibility and eosinophilic inflammation and the patients with COPD those present reversibility and eosinophilic inflammations and give a response to the steroids lead to difficulties in the disease management.
Inflammation features of these 3 groups are seen in Table 3 (5).

As it is seen from the table, late onset asthma shows more similarities with the early onset asthma. Neutrophilic inflammation and loss of the reversibility in the early onset and aged asthmatics are remarkable.
Diagnostic Methods
Because of the above mentioned reasons, anamnesis, physical examination, pulmonary function test and reversibility tests, bronchial provocation test and allergy tests those can be sufficient for the classical asthma diagnosis may not be always sufficient for the diagnosis of the elderly asthmatics.
In addition to these, full blood count (for anemia and infection), chest radiography, electrocardiography (a very high negative predictive value for the heart failure), blood gas, body plethysmography and diffusion capacity measurement, induced sputum cell count, exhaled NO measure (FeNO), high resolution computed tomography and bronchoalveolar lavage may be needed (1,11).
Spirometry
The spirometric values are characteristic in the elderly. Age related changes can mimic the obstructive pulmonary diseases and FEV1/FVC may be < 70% even in the healthy, nonsmoker asymptomatic persons (1). FEV1/FVC rate < 70% which is used for diagnosis of the pulmonary diseases is not valid in the elderly. Reference spirometry values are different in the elderly. FEV1/FVC rate is 75-64% for 65 years old and 67-56% for 85 years old. Using of the post-bronchodilator FEV1/FVC rate is important to prevent the false positivity. The post-bronchodilator rate is never < 71% in the healthy individuals. One out of every 5 elderly asthmatic (19.5%) is misdiagnosed as COPD (15).
In a study with 597 patients previously diagnosed as asthma or chronic bronchitis or prescribed in this way, the patients were re-evaluated with post-bronchodilator FEV1/FVC rate and 235 patients of them (39.4%) were diagnosed with COPD. On the previous diagnoses, 121 (51.5%) of these patients were seen to be misdiagnosed as asthma (14).
Furthermore, LLN (lower limit of normal) which is calculated statistically with confidence interval and 5th percentile is recommended to be used. The discordance of FEV1/FVC with LLN is 7.5%. The discordance rate increases particularly in very long-short and very older-young groups. Therefore, use of LNN in the elderly will be appropriate.
Asthma COPD differentiation using post-bronchodilator FEV1/FVC and reversibility is summarized in Table 4 (14,16).

Reversibility Test
Because of the impairment in the functions of beta-adrenergic receptors and since the same impairment is not seen in the cholinergic receptors, the test should be done with both the agents. An ultimate increase of the FEV1 ≥ % 15 with 400 mg salbutamol spacer or 2.5 mg nebulizer for the early reversibility and with 30 mg/day prednisolone for 14 days for the late reversibility is considered as positive. It should be remembered the reversibility will be less in the chronic asthmatics (5).
PEF Variability
This is not significant for the elderly since the pathology is more in the small air ways. PEF variability decreases by age due to reasons such as the increase in the chest wall rigidity, muscle weakness and lack of coordination, but the negative PEF does not exclude the asthma (5).
Bronchial Provocation Test
This test has a very high negative predictive value in the diagnosis of asthma. BHR increases from 10-16% to 29-43% by age, but it is not helpful after the development of the fixed air way obstruction (5,11).
Skin Test
The positivity increases by age. It decreases from 78.7% between 6 and 34 years old to 39.6% after 55 years old (17).
CONCLUSION
Tiring the patient out in the elderly with such detailed examinations can be discussed, and some authors advocate a more conservative approach. However, control of the inflammation gains quite importance. Therefore, achieving the most accurate diagnosis with the minimal aggressive approach as much as possible should be targeted. In the clinical studies, this age group is always excluded, and the real life diagnosis and treatment studies specific to this group are urgently needed.
CONFLICT of INTEREST
None declared.
REFERENCES
- Barua P, O'Mahony MS. Overcoming gaps in the management of asthma in older patients drugs aging 2005; 22: 1029-59. [?zet]
- Goeman DP, Douglass JA. Optimal management of asthma in elderly patients strategies to improve adherence to recommended interventions. Drugs Aging 2007; 24: 381-94. [?zet]
- Jones SC, Iverson D, Burns P, Evers U, Caputi P, Morgan S. Asthma and ageing: an end user's perspective-the perception and problems with the management of asthma in the elderly. Clin Exp Allergy 2011; 41: 471-81. [?zet]
- Bom AT, Pinto AM. Allergic respiratory diseases in the elderly. Respir Med 2009; 103: 1614-22. [?zet]
- Lindner K, Panaszek B, Machaj Z. Asthma in the elderly. Pol Arch Med Wewn 2007; 8: 350-4. [?zet]
- Sin BA, Akkoca O, Saryal S, Oner F, Misirligil Z. Differences between asthma and COPD in the elderly. J Investig Allergol Clin Immunol 2006; 16: 44-50. [?zet] [PDF]
- Dahlberg PE, Busse WW. Is intrinsic asthma synonymous with infection? Clin Exp Allergy 2009; 39: 1324-9. [?zet]
- King MJ, Hanania NA. Asthma in the elderly: current knowledge and future directions. Curr Opin Pulm Med 2010; 16: 55-9. [?zet]
- Yilmaz S, Ekici A, Ekici M, Kele H. High-resolution computed tomography findings in elderly patients with asthma. Eur J Radiol 2006; 59: 238-43. [?zet]
- Kuebler KK, Buchsel PC, Balkstra CR. Differentiating chronic obstructive pulmonary disease from asthma. J Am Acad Nurse Pract 2008; 20: 445-54. [?zet]
- Di Lorenzo G, Mansueto P, Ditta V, Esposito-Pellitteri M, Lo Bianco C, Leto-Barone MS, et al. Similarity and differences in elderly patients with fixed airflow obstruction by asthma and by chronic obstructive pulmonary disease. Respir Med 2008: 102; 232-8. [?zet]
- Fabbri LM, Romagnoli M, Corbetta L, Casoni G, Busljetic K, Turato G, et al. Differences in airway inflammation in patients with fixed airflow obstruction due to asthma or chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2003; 167: 418-24. [?zet] [Tam Metin] [PDF]
-
Urso DL. Asthma in the elderly. Curr Gerontol Geriatr Res 2009. Epub 2009 Oct 27.
[?zet] [Tam Metin] [PDF] - Tinkelman DG, Price DB, Nordyke RJ, Halbert RJ. Misdiagnosis of COPD and asthma in primary care patients 40 years of age and over. J Asthma 2006; 43: 75-80. [?zet]
- Bellia V, Battaglia S, Catalano F, Scichilone N, Incalzi RA, Imperiale C, et al. Aging and disability affect misdiagnosis of COPD in elderly asthmatics. Chest 2003; 123: 1066-72. [?zet] [Tam Metin] [PDF]
- Bhatt NY, Wood KL. What defines abnormal lung function in older adults with chronic obstructive pulmonary disease? Drugs Aging 2008; 25: 717-28. [?zet]
- Burrows B, Martinez FD, Halonen M, Barbee RA, Cline MG. Association of asthma with serum IgE levels and skin-test reactivity to allergens. N Engl J Med 1989; 320: 271-7. [?zet]
Yaz??ma Adresi (Address for Correspondence):
Dr. Ay??n ?akar CO?KUN,
Celal Bayar ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
MAN?SA - TURKEY
e-mail: aysins@hotmail.com