Y?ksek doz lipozomal amfoterisin B ile k?r sa?lanan ?ocukluk ?a?? invaziv mukormikozis
Fatih
ERBEY1, Emine KOCABA?2, ?brahim BAYRAM1,
S?reyya SOYUPAK3, Derya G?M?RD?L?4,
Atila TANYEL?1
1 ?ukurova ?niversitesi T?p Fak?ltesi, ?ocuk Sa?l??? ve Hastal?klar? Anabilim Dal?,
?ocuk Onkoloji Bilim Dal?, Adana,
2 ?ukurova ?niversitesi T?p Fak?ltesi, ?ocuk Sa?l??? ve Hastal?klar? Anabilim Dal?,
?ocuk ?nfeksiyon Bilim Dal?, Adana,
3 ?ukurova ?niversitesi T?p Fak?ltesi, Radyoloji Anabilim Dal?, Adana,
4 ?ukurova ?niversitesi T?p Fak?ltesi, Patoloji Anabilim Dal?, Adana.
?ZET
Y?ksek doz lipozomal amfoterisin B ile k?r sa?lanan ?ocukluk ?a?? invaziv mukormikozis
Pulmoner mukormikozis medikal tedavisinin temel dayana?? amfoterisin B olup, optimal doz konusunda hen?z bir fikir birli?i bulunmamaktad?r. Bu yaz?da pulmoner mukormikozis geli?en akut lenfblastik l?semili bir olgunun 45 haftal?k s?rede toplam 42.55 g lipozomal amfoterisin B kullan?larak ba?ar?yla tedavi edildi?i sunulmaktad?r. T?bbi literat?re bak?ld???nda bu olgu ?ocukluk ?a??nda en y?ksek dozda lipozomal amfoterisin B'nin ba?ar?yla kullan?ld??? ilk olgudur.
Anahtar Kelimeler: Lipozomal amfoterisin B, invaziv pulmoner mantar infeksiyonu, ?ocukluk ?a??.
SUMMARY
Pediatric invasive mucormycosis cured with high dose liposomal amphotericin B
Fatih
ERBEY1, Emine KOCABA?2, ?brahim BAYRAM1,
S?reyya SOYUPAK3, Derya G?M?RD?L?4,
Atila TANYEL?1
1 Division of Pediatric Oncology, Faculty of Medicine, Cukurova University, Adana, Turkey,
2 Division of Pediatric Infectious, Faculty of Medicine, Cukurova University, Adana, Turkey,
3 Department of Radiology, Faculty of Medicine, Cukurova University, Adana, Turkey,
4 Department of Pathology, Faculty of Medicine, Cukurova University, Adana, Turkey.
Amphotericin B remains the mainstay medical treatment of pulmonary mucormycosis. Optimal dose is not defined. We described a case of pulmonary mucormycosis, which had been treated with 42.55 g (during to 45 weeks) liposomal amphotericin B. In medical literature this case is one of the highest doses of lyposomal amphotericin B administered to a pediatric patient.
Key Words: Liposomal amphotericin B, invasive pulmonary fungal infection, childhood.
Geli? Tarihi/Received: 31/08/2010 - Kabul Edili? Tarihi/Accepted: 04/01/2011
INTRODUCTION
Mucormycosis is the third most common invasive fungal infection after aspergillosis and candidiasis (1,2). It represents 8.3-13% of all fungal infections encountered during the autopsy of leukemia, lymphoma patients (3,4). Major forms of infection are, rhino-orbito-cerebral, pulmonary, disseminated, cutaneous, and gastrointestinal. Mucormycosis occurs most frequently in patients with ketoacidotic diabetes, acute leukemia or lymphoma who are neutropenic, and in transplanted patients receiving immunosuppressive treatment (5,6,7). Amphotericin B is used in the medical treatment of mucor for 2 or 3 months at a dose of 1-3 mg/kg/day (8). The dose should be initiated as at least 5 mg/kg/day if an invasive pulmonary fungal infection is suspected, and it should be increased according to the patient response. Here we describe a case of pulmonary mucormycosis which had been treated with 42.55 g (during to 45 weeks) lyposomal amphotericin B. In medical literature this case is one of the highest doses of lyposomal amphotericin B administered to a pediatric patient.
CASE REPORT
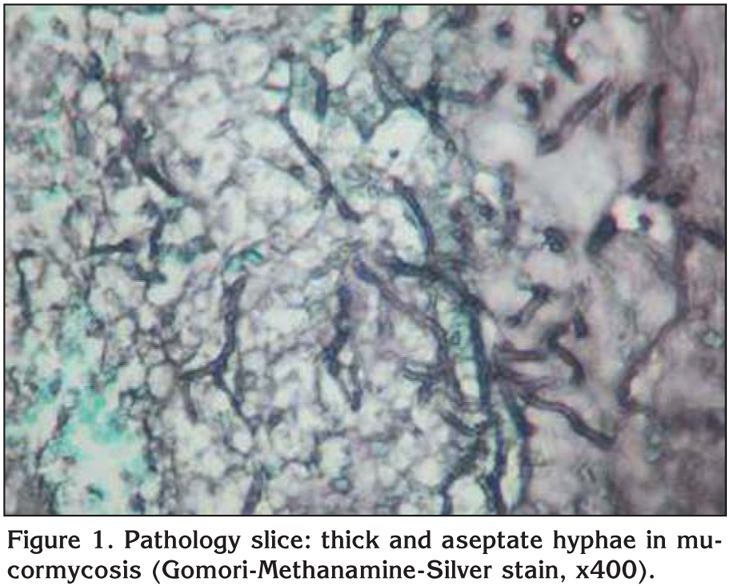
A 9-years-old male patient followed up with the diagnosis of acute lymphoblastic leukemia-L1 (ALL-L1). The patient was admitted with complaints of fever and swelling of the cheek on the 8th month of his induction chemotherapy (BFM, TRALL-2000). On his physical examination it was determined that he had oral aphthous lesions and swelling of one cheek. Lung auscultation findings and examinations of other systems proved normal. He received 10 mg/m2/day dexamethasone, 1.5 mg/m2 vincristine once a week, 30 mg/m2 doxorubicin once a week and 10.000 U/m2 L-asparaginase for 4 days within the last month. Laboratory results of the patient were: total white blood cell (WBC) count 800/mm3, absolute neutrophile count (ANC) 200/mm3, Hct: 25%, thrombocytes 55.000/mm3. Level of Na was 138 mmol/L, K 4.0 mmol/L, BUN 15 mg/dL, Cr 0.8 mg/dL, ALT 38 U/L, AST 42 U/L, serum reactive protein (CRP) 181 mg/L, and procalcitonin (PCT) 0.89 ng/mL. Meropenem was initiated according to the febrile neutropenia (FEN) protocol. Vancomycin was added to the treatment on the 3rd day of hospitalization since fever did not decrease (38.5?C). Maxillofacial tomography of the patient was taken, the aphthous lesions of the patient persisted and swelling in the cheek became more significant. Tomography revealed no findings other than soft tissue edema. Amphotericin B deoxycholate (1 mg/kg/day) was added to the treatment of the patient with ongoing fever. Fever was controlled in the follow up of the patient, but WBC count increased up to 10.000/mm3 (duration of total neutropenia was 5 days). However black plaques and lesions with tendency for necrosis were determined in the palate and right upper gums. Lesions were debrided and sent for pathologic examination. The patient developed tachypnea on the 14th day of his follow up and coarse crackles were auscultated in his lungs. Biopsy material obtained from palate showed thick and aseptate hyphae after staining with Gomori-Methanamine-Silver stain (Figure 1). Thorax tomography was obtained. Several and various, patchy, nodular opacities with tendency to become peripheral were noted in the lung parenchyma (Figure 2). This image, radiologically conformed to mucormycosis. Amphotericin B deoxycholate therapy was stopped on day 14 and lyposomal amphotericin B (AmBisome) at a dose of 5 mg/kg/day was started. The patient was followed up with his clinic and thorax tomography. Intermittent bone marrow aspirations were performed and no active chemotherapies were administered during the period of remission. The thorax tomography obtained on day 73 of the therapy showed progression in the number and size of the lesions compared to the results of the tomography taken on day 40. Meanwhile the patient had no complaints including fever and cough. Auscultation revealed coarse crackles in the lungs. Laboratory findings of the patient were: WBC count 8800/mm3, ANC 4800/mm3, Hct: 29%, thrombocytes 185.000/mm3. Level of Na was 136 mmol/L, K 3.6 mmol/L, BUN 11 mg/dL, Cr 0.5 mg/dL, ALT 28 U/L, AST 40 U/L, CRP 21 mg/L, and PCT 0.15 ng/mL. The dose of liposomal amphotericin B was gradually increased up to 10 mg/kg. Maintenance chemotherapy (6-mercaptopurin 50 mg/m2/day and methotrexate 20 mg/m2/week) was initiated at half dose at week 20 of lyposomal amphotericin B therapy for the risk of a possible ALL relapse. The total dose was attained one month after the start of the maintenance chemotherapy. However 2 weeks later, the patient began to cough and coarse crackles were auscultated in the lungs. Maintenance chemotherapy was stopped and ceftazidime + amikacin were added to lyposomal amphotericin B therapy when WBC count became 2000/mm3, and ANC decreased to 200/mm3. Ceftazidime + amikacin therapy was completed to 14 days and then stopped, the neutropenia of the patient lasted 6 days and auscultation findings improved. Thorax tomography obtained in this period showed no changes in the number and size of the lesions. The patient had no additional complaints during the continuation of lyposomal amphotericin B therapy. Thorax tomography obtained at week 45 of the therapy showed that lesions had disappeared completely and thus lyposomal amphotericin B therapy was discontinued. Patient received a total of 42.55 g of lyposomal amphotericin B therapy over a 45-week period. No side effects associated with lyposomal amphotericin B were determined during this period. Parenchymal lesions observed previously had disappeared in the thorax tomography of the patient that was obtained 3 months later (Figure 3). The patient is still followed up by our department and is receiving maintenance chemotherapy for ALL since the last 18 months.


DISCUSSION
Mucormycosis is a rare fungal infection that affects almost all immunocompromised patients. Pulmonary is the second most common involvement after rhinocerebral disease. Leukemia and lymphoma are major risk factors for mucormycosis. The diagnosis of mucormycosis is particularly difficult in immunocompromised patients. Even in the presence of hematogenous dissemination of fungi, blood cultures are negative (9). Therefore, tissue biopsy and histologic identification of fungi remain the gold standard of diagnosis. But the diagnosis is often made after death (3). Prognosis is poor and overall mortality is high (5,7). Our patient had major risk factors for the development of mucor including acute leukemia, neutropenia, and had received intensive chemotherapy and the diagnosis was established by the debridement of black plaques in the palate with tendency for necrosis and histopathological examination of the debridement material.
Pulmonary mucormycosis, is the second most common site of involvement of mucorales infection. Inhalation of spores is the primary route of infection. Patients with leukaemia, lymphoma and severe neutropenia remain at greater risk of developing pulmonary mucormycosis compared to other forms (1,6). Patients can show symptoms of cough, fever, haemoptysis and pleuritic chest pain (4,7). Radiological findings include infiltrate, wedge-shaped consolidation, nodule, cavitation, mycetoma, lobar collapse and, rarely pleural effusion (1,4,7). The establishment of mucor in the debridement material obtained from the palate of our patient, the development of respiratory system symptoms despite the administration of a broad spectrum antibiotics and the observation of several, various, parenchymal patchy nodular opacities with a tendency to become peripheral in thorax tomography, suggested that this pathology was most probably pulmonary mucormycosis. However, pulmonary biopsy could not be performed due to the poor general condition of the patient as well as the wide dispersion of the lesions.
Therapy of mucormycosis is based on three approaches: rapid control of the patient's underlying predisposing condition, antifungal therapy and surgical debridement. Tedder et al. in a review of 255 cases of pulmonary mucormycosis, who reported that the mortality rate was significantly lower for patients who underwent surgery than for those who received medical treatment only (9.4% vs. 50%, p= 0.01) (10). We were able to perform debridement from only the palate lesions of our patient, and could not perform surgical debridement from the pulmonary lesions for their wide dispersion.
Amphotericin B remains the mainstay medical treatment of pulmonary mucormycosis. Optimal dose is not defined. Generally dose of amphotericin B, 1-3 mg/kg/day, and minimum of 6 weeks of treatment has been recommended (8,11). Ringden et al. found lung tissue concentrations of amphotericin B to be lower than those in other tissues, suggesting that pulmonary fungal infections may require higher dosage of amphotericin B (12). The use of high doses of amphotericin B has been correlated with a good prognosis (5). Therefore, when an invasive fungal infection is suspected it should be started at a minimum dose of 5 mg/kg/day and increased according to the patient response. Cagatay et al. have reported that they succeeded curing a 31 years old male diabetic patient with the administration of a total of 32 g of lyposomal amphotericin B for 6 months (13). Donado-Una et al. treated a pulmonary mucormycosis infection in a 67 years old male diabetic patient with a total of 28.7 g of lyposomal amphotericin B (11). Maury et al. on the other hand, achieved success in the treatment of a 3 years old ALL patient who had developed disseminated mucormycosis with a total of 27 g of lyposomal amphotericin B (14). Mondy et al. also treated a 50 years old, female diabetic patient with rhinocerebral mucormycosis infection with cumulative 126.3 g of amphotericin B lipid complex administered intermittently over a period of 16 months (15). Our patient is the first pediatric case in medical literature that was diagnosed with childhood invasive mucor infection and successfully treated with cumulative 42.55 g of lyposomal amphotericin B over a period of 45 weeks. The patient tolerated lyposomal amphotericin B treatment well. Fever, chills, nausea, or renal dysfunction was not observed at any time during the therapy. Low dose oral potassium supplementation was used to preserve a normal serum level.
Consequently, a pediatric ALL case with very high mortality invasive pulmonary mucormycosis infection was successfully treated with a high dose lyposomal amphotericin B. This is the highest dose administered in medical history in the pediatric age group.
CONFLICT of INTEREST
None declared.
REFERENCES
- Prabhu RM, Patel R. Mucormycosis and entomophthoramycosis: a review of the clinical manifestations, diagnosis and treatment. Clin Microbiol Infect 2004; 10 (Suppl 1): 31-47.
- Eucker J, Sezer O, Graf B, Possinger K. Mucormycoses. Mycoses 2001; 44: 253-60.
- Nosari A, Oreste P, Montillo M, Carrafiello G, Draisci M, Muti G, et al. Mucormycosis in hematologic malignancies: an emerging fungal infection. Haematologica 2000; 85: 1068-71.
- Funada H, Matsuda T. Pulmonary mucormycosis in a hematology ward. Intern Mewd 1996; 35: 540-4.
- Pagano L, Ricci P, Tonso A, Nosari A, Cudillo L, Montillo M, et al. Mucormycosis in patients with haematological malignancies: a retrospective clinical study of 37 cases. GIMEMA Infection Program (Gruppo Italiano Malattie Ematologiche Maligne dell'Adulto). Br J Haematol 1997; 99: 331-6.
- Ribes JA, Vonover-Sams CL, Baker DJ. Zygomycetes in human disease. Clin Microbiol Rev 2000; 13: 236-301.
- Lee FY, Mossad SB, Adal KA. Pulmonary mucormycosis: the last 30 years. Arch Intern Med 1999; 159: 1301-9.
- Chopra R. Ambisome in the treatment of fungal infections. The UK experience. J Antimicrob Chemother 2002; 49: 43-7.
- Richardson M, Ellis M. Clinical and laboratory diagnosis. Hosp Med 2000; 61: 610-4.
- Tedder M, Spratt JA, Anstadt MP, Hegde SS, Tedder SD, Lowe JE. Pulmonary mucormycosis: results of medical and surgical therapy. Ann Thorac Surg 1994; 57: 1044-50.
- Donado-Una JR, Diaz-Hellin V, Lopez-Encuentra A, Echave-Sustaeta JM. Persistent cavitations in pulmonary mucormycosis after apparently successful amphotericin B. Eur J Cardiothorac Surg 2002; 21: 940-2.
- Ringden O, Meunier F, Tollemar J, Ricci P, Tura S, Kuse E, et al. Efficacy of amphotericin B encapsulated in liposomes (AmBisome) in the treatment of invasive fungal infections in immunocompromised patients. J Antimicrob Chemother 1991; 28(Suppl B): 73-82.
- Cagatay AA, Onc? SS, Calangu SS, Yildirmak TT, Ozs?t HH, Eraksoy HH. Rhinocerebral mucormycosis treated with 32 gram liposomal amphotericin B and incomplete surgery: a case report. BMC Infect Dis 2001; 1: 22.
- Maury S, Leblanc T, Feuilhade M, Molina JM, Schaison G. Successful treatment of disseminated mucormycosis with liposomal amphotericin B and surgery in a child with leukemia. Clin Infect Dis 1998; 26: 200-2.
- Mondy KE, Haughey B, Custer PL, Wippold FJ 2nd, Ritchie DJ, Mundy LM. Rhinocerebral mucormycosis in the era of lipid-based amphotericin B: case report and literature review. Pharmacotherapy 2002; 22: 519-26.
Yaz??ma Adresi (Address for Correspondence):
Dr. Fatih ERBEY,
?ukurova ?niversitesi T?p Fak?ltesi,
?ocuk Sa?l??? ve Hastal?klar? Anabilim Dal?,
?ocuk Onkoloji Bilim Dal?,
01330 ADANA - TURKEY
e-mail: erbeyfa@gmail.com