?ok nadir bir plevran?n ?o?ul kalsifiye t?m?r? olgusu
Yetkin A?A?KIRAN1, G?kt?rk FINDIK2, Koray AYDO?DU2, Ersin G?NAY3, Sibel G?NAY3, Sadi KAYA2
1 SB Atat?rk G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi, Patoloji Klini?i, Ankara,
2 SB Atat?rk G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi, G???s Cerrahisi Klini?i,
Ankara,
3 SB Atat?rk G???s Hastal?klar? ve G???s Cerrahisi E?itim ve Ara?t?rma Hastanesi, G???s Hastal?klar? Klini?i,
Ankara.
?ZET
?ok nadir bir plevran?n ?o?ul kalsifiye t?m?r? olgusu
Kalsifiye fibr?z t?m?rler nadir lezyonlard?r. Bu lezyonlar psammoma benzeri lenfoplazmositer infiltrasyon ve yayg?n distrofik kalsifikasyonlar i?eren hiyalinize kollajen?z fibrotik dokulardan olu?maktad?r. Plevran?n kalsifiye fibr?z t?m?rleri nadiren sunulmu?tur. ?o?ul plevran?n kalsifiye fibr?z t?m?rleri son derece nadiren bildirilmi?tir. K?rk ya??nda erkek hasta klini?imize nefes darl??? ?ikayetiyle ba?vurdu. Toraks bilgisayarl? tomografisinde en geni? ?ap? 2 cm olan plevral yerle?imli ?o?ul yumu?ak doku olu?umlar? izlenmesi ?zerine cerrahi giri?im planland?. Video yard?ml? torakoskopik cerrahi ile al?nan frozen plevra biyopsisi kesitleri kalsifiye fibr?z t?m?r olarak raporland?. Lezyonlar?n ?ok say?da olmas? ve plevral yap???kl?klar?n bulunmas? nedeniyle k?ratif plevral dekortikasyon uyguland?. Olgu, ?o?ul plevran?n kalsifiye fibr?z t?m?rlerinin son derece nadir olmas? nedeniyle sunuldu.
Anahtar Kelimeler: Kalsifiye fibr?z t?m?r, ?o?ul, plevra.
SUMMARY
An extremely rare case of multiple calcifying tumor of the pleura
Yetkin A?A?KIRAN1, G?kt?rk FINDIK2, Koray AYDO?DU2, Ersin G?NAY3, Sibel G?NAY3, Sadi KAYA2
1 Clinic of Pathology, Ataturk Chest Diseases and Chest Surgery Training and Research Hospital,
Ankara, Turkey,
2 Clinic of Chest Surgery, Ataturk Chest Diseases and Chest Surgery Training and Research Hospital,
Ankara, Turkey,
3 Clinic of Chest Diseases, Ataturk Chest Diseases and Chest Surgery Training and Research Hospital,
Ankara, Turkey.
Calcifying fibrous tumors are uncommon lesions. These lesions are made up of hyalinized collagenous fibrotic tissues interspersed with lymphoplasmacytic infiltrates and extensive dystrophic calcifications mimicking psammomatous features. Calcifying tumor of pleura is rarely presented. Multiple calcifying tumor of pleuras have been reported extremely seldom. Forty-year-old male patient was admitted to our clinic with complaints of dyspnea. Because of the multiple soft tissue formations at the pleural region with the largest diameter of 2 cm on thorax computed tomography, surgical intervention was planed. Frozen sections of pleural biopsies that were taken during video-assisted thoracoscopic surgery were reported as calcifying fibrous tumor. Because of the presence of multiple lesions and pleural adhesions, curative pleural decortication was performed. This case is presented with extremely rare entity of multiple calcifying tumor of plevras.
Key Words: Calcifying fibrous tumor, multiple, pleura.
Geli? Tarihi/Received: 07/03/2012 - Kabul Edili? Tarihi/Accepted: 15/05/2012
INTRODUCTION
Calcifying fibrous tumors are rare lesions. These lesions consist of hyalinized collagenous fibrotic tissues interspersed with lymphoplasmacytic infiltrates and extensive dystrophic calcifications, often with psammomatous features (1,2,3). Most cases occur in children and young adults with no sex predilection. Calcifying fibrous tumors occur more often in the soft tissues of the extremites, trunk, neck, scrotum, groin or axilla. However, seldom cases have been reported in the mediastinum, pleura, and visceral peritoneum (4,5,6,7).
Originally, Rosenthal and Abdul-Karim described calcifying fibrous tumors as a "childhood fibrous tumor with psammoma bodies" in 1988 (8). In 1993, Fetsch et al. reported ten additional cases and re-named the entity as calcifying fibrous pseudotumor (CFP) (9). In the recently published classification of the World Health Organization (WHO), the term of calcifying tumor of the pleura (CTP) is used for this entity (10).
In the literature, we could find only 11 reported cases of CTP. Because of the presence of multiple CTP, we reported this case with its rare entity.
CASE REPORT
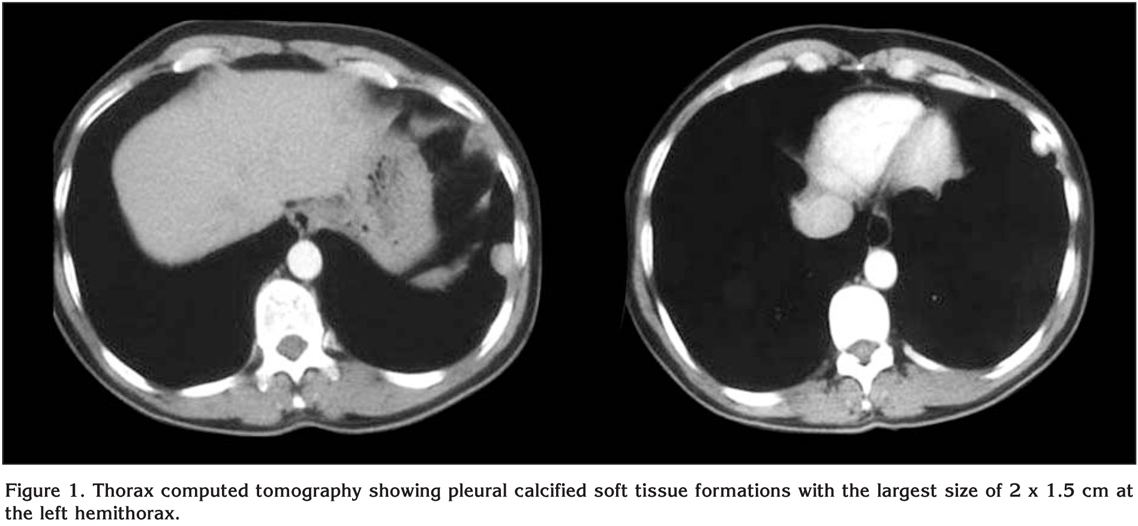
A 40-year-old male patient was admitted to our clinic with the complaints of gradually increasing dyspnea of recent onset. On his physical examination, vital signs were in normal limits. Respiratory system examination revealed decreased respiratory sounds and dull percussion over left hemi-thorax. Other system examinations were unremarkable. Laboratory examinations revealed slightly elevated serum ALT and AST levels. All the other laboratory results were in normal limits. Spirometry was revealed normal respiratory functions [FEV1: 3.26 (80% of predicted), FVC: 4.5 (83% of predicted), and FEV1/FVC: 80%]. Thorax computed tomography (CT) showed multiple soft tissue formations including calcifications with the largest diameter of 2 cm at the level of left lingular and left basal segments (Figure 1). There was no pathological lymph nodes in the mediastinum.
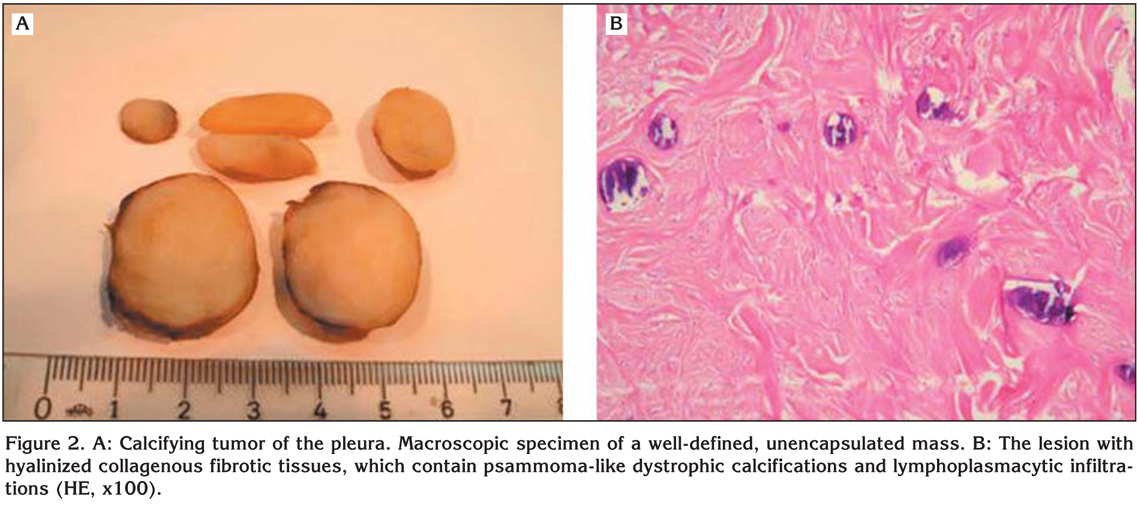
Video-assisted thoracoscopic surgery (VATS) was performed for monitoring the pleural lesions. Thoracoscopic examination demonstrated two well-defined pleural lesions on the lateral wall of the left hemithorax and extensive pleural adhessions. A biopsy specimen was obtained and sent for the frozen section examination. The frozen section revealed a benign/calcifying tumor. In order to achive an exact diagnosis, curative treatment, and presence of pleural adhessions, left thoracotomy was performed instead of VATS. The left hemi-thorax could be visualized via left thoracotomy incision through the 5th intercostal space. In the detailed examination, four lesions of pleural origin were detected. Each lesions were removed by pleural decortication. No lesion was palpated in the lung paranchyme. Macroscopical evaluation revealed 4 well-defined, unencapsulated masses, the largest of which was nearly 2.2 x 1.5 x 1 cm in diameter (Figure 2A). Histopathological examination of all these lesions were revealed the diagnosis of "CTP" with psammomatous calcifications and lymphohistiocytic inflammatory cell infiltrations in hyalinized collogenous fibrotic tissue (Figure 2B). In the immunohistochemical staining, the fibrous tissue was positive for vimentin and inflammatory cells were positive for CD45 and CD68. However, it was stained negative for actin, desmin, S100 protein, CD31, and CD34. Also, no positive staining was determined in the controlled histochemical staining for amiloid. All chest tubes of the patient were removed at the postoperative 1st and 3rd days. No complications were observed, and the patient was discharged at the end of the postoperative 1st week.
DISCUSSION
Calcifying fibrous tumor is a rare benign soft tissue entity with unique histologic features originally reported by Rosenthal and Abdul-Karim as a pediatric fibrous tumor with psammoma bodies in 1988 (8). In 1993, Fetsch et al. reported an analysis of 10 additional cases and re-named the entity as calcifying fibrous pseudotumor (9). In the recently published classification of the WHO for tumors of the lung, pleura, thymus and heart, the term of CTP is suggested for this entity (10).
Calcifying fibrous tumors are uncommon lesions and usually found in children and young adults with no sex predilection (5). Calcifying fibrous tumors more often occur in the soft tissues of the extremites, trunk, neck, scrotum, groin or axilla. However, pleural or mediastinal involvements are extremly rare reported localizations for calcifying fibrous tumor (5). In the literature, we could find only a few multiple CTP cases (1,3,4).
Calcifying fibrous tumors are generally solitary lesions. Their etiology or pathogenesis has not been defined. The complaint upon presentation is usually nonspecific pain. The lesions are unencapsulated and originate from parietal or visceral pleura (2,5,10). In the literature, we could find 11 reported cases of CTP. With respect to number of the nodules, distribution of these cases was described as 4 multiple, 4 solitary, 2 disseminated and 1 bilateral lesions (1,2,3,4,5,11,12,13). In our case, CTP was in the form of multiple lesions located in the left hemithorax and treated with total decortication.
Histologically, calcifying fibrous tumor consists of hyalinized collagenous fibrotic tissues interspersed with lymphoplasmatic infiltrates and extensive dystrophic calcifications, often with psammomatous features (6).
CTPs have to be differentiated from other pleural lesions such as solitary fibrous tumor (SFT), calcified granulomas, calcified pleural plaques and chronic fibrous pleuritis (3,4,5,6). In the differential diagnosis, immunohistochemically, SFTs are often positively stained with CD34 and do not contain extensive dystrophic calcifications. In calcified granulomas, residual histiocytes and multinuclear giant cells are present. It should be kept in mind that calcified pleural plaques and calcified chronic fibrous pleuritis contain diffuse pleural thickening that can not form a pleural mass.
CTPs are often confused with intrapulmonary lesions such as hyalinized granulomas, inflammatory myofibroblastic tumors, and amyloid (5,7,10). Inflammatory myofibroblastic tumors are positive for vimentin as well as for smooth muscle actin and rarely for desmin. Hyalinized granulomas, however, involve foreign body response areas around central keloid-like hyalinized collagen. This appearance usually mimics nodular amiloidosis, but with specific stains, they are amyloid negative which is differential characteristics for hyalinized granulomas. Amiloidosis can be diagnosed via specific histochemical staining.
Calcification characteristics of CTPs cannot be shown through standard posterior-anterior and lateral chest X-rays, although they can be evaluated in detail through with thorax computed tomography. Closed pleural biopsies and thoracoscopic pleural biopsies can be used for diagnostic purposes. However, the principal method of treatment is complete resection with open surgery (5,7). In the literature, complete resection was performed for 9 of 11 cases and no recurrence has been reported. Thoracoscopic complete resection also reported (2). In case of incomplete resection, tumor continues to grow, and thus, a second operation may be needed (3).
Multiple CTPs are uncommon pleural lesions. They should be differentiated from pleural lesions such as solitary fibrous tumors, calcified granulomas, calcified pleural plaques and chronic fibrous pleuritis as well as intrapulmonary lesions such as hyalinizing granuloma, inflammatory pseudotumour and amyloid (14). Thoracoscopic interventions can be sufficient for diagnosis. However, the principal treatment method is open surgery because the total excision of the lesions even that cannot be radiologically imaged can be achieved.
CONFLICT of INTEREST
None declared.
REFERENCES
- Mito K, Kashima K, Daa T, Kondoh Y, Miura T, Kawahara K, et al. Multiple calcifying fibrous tumors of the pleura. Virchows Arch 2005; 446: 78-81.
- Ammar A, El Hammami S, Horchani H, Sellami N, Kilani T. Calcifying fibrous pseudotumor of the pleura: a rare location. Ann Thorac Surg 2003; 76: 2081-2.
- Shibata K, Yuki D, Sakata K. Multiple calcifying fibrous pseudotumors disseminated in the pleura. Ann Thorac Surg 2008; 85: 3-5.
- Kawahara K, Yasukawa M, Nakagawa K, Katsura H, Nagano T, Iwasaki T. Multiple calcifying fibrous tumor of the pleura. Virchows Arch 2005; 447: 1007-8.
- Jang KS, Oh YH, Han HX, Chon SH, Chung WS, Park CK, et al. Calcifying fibrous pseudotumor of the pleura. Ann Thorac Surg 2004; 78: e87-8.
- Jeong HS, Lee GK, Sung R, Ahn JH, Song HG. Calcifying fibrous pseudotumor of mediastinum--a case report. J Korean Med Sci 1997; 12: 58-62.
- Nascimento AF, Ruiz R, Hornick JL, Fletcher CD. Calcifying fibrous 'pseudotumor': clinicopathologic study of 15 cases and analysis of its relationship to inflammatory myofibroblastic tumor. Int J Surg Pathol 2002; 10: 189-96.
- Rosenthal NS, Abdul-Karim FW. Childhood fibrous tumor with psammoma bodies. Clinicopathologic features in two cases. Arch Pathol Lab Med 1988; 112: 798-800.
- Fetsch JF, Montgomery EA, Meis JM. Calcifying fibrous pseudotumor. Am J Surg Pathol 1993; 17: 502-8.
- Travis WD, Tazelaar H, Churg A, et al. Mesenchymal tumours. In: Travis WD, Brambilla E, M?ller-Hermelink HK, Harris CC (eds). World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. Lyon: IARC Press, 2004: 141-4.
- Pinkard NB, Wilson RW, Lawless N, Dodd LG, McAdams HP, Koss MN, et al. Calcifying fibrous pseudotumor of pleura. A report of three cases of a newly described entity involving the pleura. Am J Clin Pathol 1996; 105: 189-94.
- Hainaut P, Lesage V, Weynand B, Coche E, Noirhomme P. Calcifying fibrous pseudotumor (CFPT): a patient presenting with multiple pleural lesions. Acta Clin Belg 1999; 54: 162-4.
- Cavazza A, Gelli MC, Agostini L, Sgarbi G, De Marco L, Gardini G. Calcified pseudotumor of the pleura: description of a case. Pathologica 2002; 94: 201-5.
- Suh JH, Shin OR, Kim YH. Multiple calcifying fibrous pseudotumor of the pleura. J Thorac Oncol 2008; 3: 1356-8.
Yaz??ma Adresi (Address for Correspondence):
Dr. Ersin G?NAY,
Afyon Kocatepe ?niversitesi T?p Fak?ltesi,
G???s Hastal?klar? Anabilim Dal?,
AFYONKARAH?SAR - TURKEY
e-mail: ersingunay@gmail.com