Eri?kin ya?ta saptanan Swyer-James-MacLeod sendromu olgusu
Nuref?an BOYACI1, ?mer KARAKA?1, Ekrem KARAKA?1, Funda YAL?IN2, Sema YILDIZ1, Hasan ?E?E1
1 Harran ?niversitesi T?p Fak?ltesi, Radyoloji Anabilim Dal?, ?anl?urfa,
2 Harran ?niversitesi T?p Fak?ltesi, G???s Hastal?klar? Anabilim Dal?, ?anl?urfa.
Tuberk Toraks 2013; 61(4): 355-356 • doi:10.5578/tt.6131
Geli? Tarihi/Received: 12/08/2013 • Kabul Edili? Tarihi/Accepted: 07/10/2013
Swyer-James-MacLeod syndrome (SJMS), or unilateral hyperlucent lung syndrome, is a rare disease thought to be associated with post-infectious bronchiolitis obliterans (1). This disease was first described in 1953 by Swyer and James in a 6-year-old child who had been treated with pneumonectomy (2). MacLeod presented a unilateral hyperlucency series one year later. From this date on, the disease was defined as Swyer-James-MacLeod syndrome (SJMS) (3). This disorder is diagnosed in children with recurrent pulmonary infection or in asymptomatic adult cases during radiological examinations. The characteristic radiological findings include unilateral air trapping, hyperlucency signs, small or normal sized lungs, and a decrease in the number and dimensions of the pulmonary vessels (3).
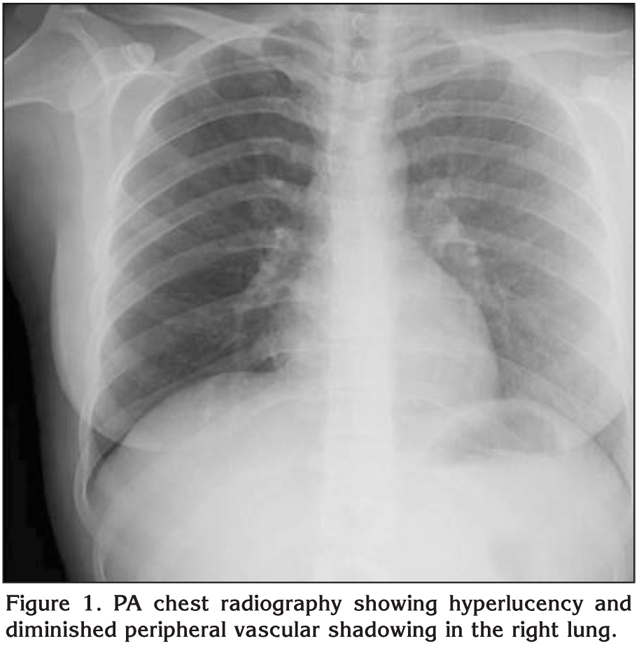
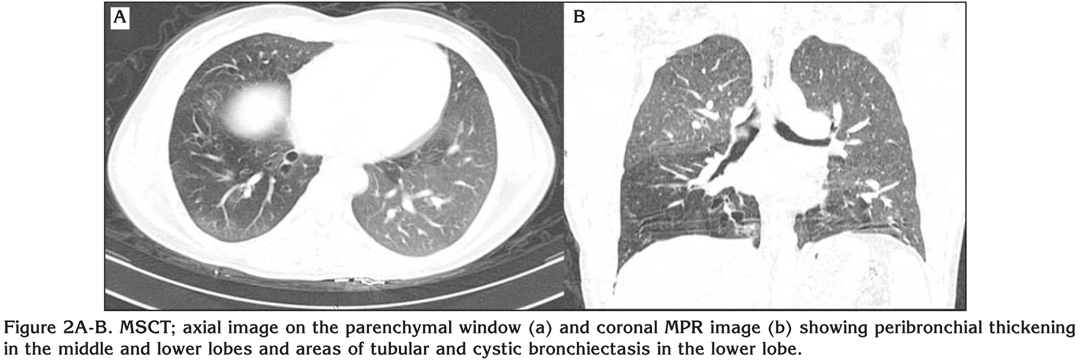
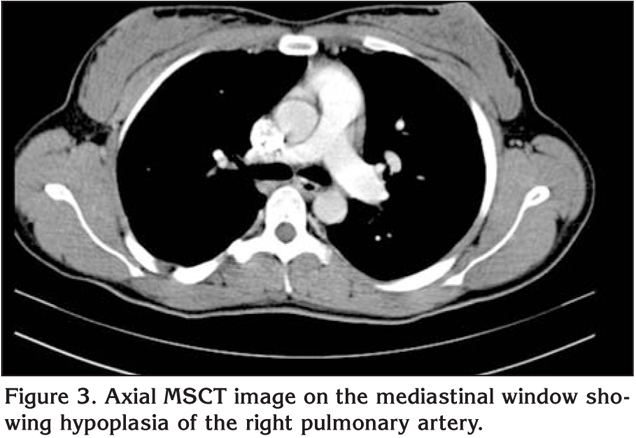
A 22-year-old female patient was admitted to our hospital with recurrent cough, wheezing and fever. The medical history of the patient included frequent recurrent attacks of bronchiolitis and particularly, productive cough triggered by infections. The physical examination of the patient revealed decreased respiratory sounds in the right lung and rare crepitant rales in the middle and lower zones, while examinations of the other systems were normal. PA chest radiography and contrast-enhanced thoracic multi-slice computerize tomography (MSCT) examinations were performed. The chest X-ray revealed hyperlucency and diminished peripheral vascular shadowing in the right lung (Figure 1). MSCT examination revealed peribronchial thickening in the right middle and lower lobe, sequelae fibrotic changes, and areas of linear and cystic bronchiectasis, which were more prominent in the lower lobe (Figure 2). The right pulmonary artery was hypoplastic (Figure 3). The findings of the bronchoscopy, performed to rule out lesions that may cause endobronchial obstruction and to investigate the presence of additional anatomical anomalies, were within normal limits.? SJMS was diagnosed on the basis of clinical findings and radiological studies.
SJMS is a type of obliterative bronchiolitis that occurs due to damage to developing lungs. In this syndrome, small bronchi and bronchioles are affected.? There is an increase in aeration of the lung areas distal to these structures due to collateral air flow.
There is hypoplasia of the lung tissue and decrease in the diameter and the number of pulmonary arteries and their branches. The decrease in perfusion and air trapping results in the finding of unilateral hyperlucent lung. The hilum of the affected lung is small, while the lung volume is normal or slightly increased. Bronchiectasis, atelectasis, and focal scars may also be observed (4).
The patients are typically asymptomatic and the disorder is frequently diagnosed accidentally on chest radiography. Unilateral air trapping on expiratory chest X-rays is the key finding.
However, the fact that unilateral hyperlucency is the most frequent finding on chest radiography is due to the rotation of the patient and it is observed with a rate of 1% on chest X-rays (5). This lucency is caused by an increase in X-ray transmission on the side to which the patient turns. This can be understood by determining if the distances between the medial ends of the clavicles and the spinous processes are equal. Moreover, unilateral hyperlucency may be caused when X-rays are not centralized and in the presence of scoliosis in the spinal column.
SJMS should always be considered in adult cases with unilateral hyperlucency on chest X-ray and a history of recurrent pulmonary infection. Evaluation of these cases by thoracic CT may prevent misdiagnosis or delayed diagnosis.
CONFLICT of INTEREST
None declared.
?REFERENCES
- Mason RJ, Murray JF, Broaddus, VC, Nadel JA. Textbook of Respiratory Medicine. 4th ed. Philadelphia: Elsevier-Saunders, 2005.
- Swyer PR, James GCA. Case of unilateral pulmonary emphysema. Thorax 1953; 8: 133-6.
- Kaplanoglu H, Kaplanoglu V, Toprak U, Dilli A, Hekimoglu B. A case of Swyer-James-Macleod syndrome associated with middle lobe hypoplasia and arteriovenous malformation. Case Rep Med 2012. doi: 10.1155/2012/ 959153.
- Lucaya J, Gartner S, Garc?a-Pe?a P, Cobos N, Roca I, Li?an S. Spectrum of manifestations of Swyer-James-MacLeod syndrome. J Comput Assist Tomogr 1998; 22: 592-7.
- Dillman JR, Sanchez R, Ladino-Torres MF, Yarram SG, Strouse PJ, Lucaya J. Expanding upon the unilateral hyperlucent hemithorax in children. Radiographics 2011; 31: 723-41.
Yaz??ma Adresi (Address for Correspondence):
Dr. Nuref?an BOYACI,
Harran ?niversitesi T?p Fak?ltesi,
Radyoloji Anabilim Dal?,
?ANLIURFA - TURKEY
e-mail: drnurefsan@yahoo.com