Ameliyat sonras? karma??k plevral yap??ma ile pn?motoraks
Hiroaki SATOH, Koichi KURISHIMA, Katsunori KAGOHASHI
Tsukuba ?niversitesi Mito T?p Merkezi, Solunum Hastal?klar? Anabilim Dal?, Ibaraki. ?
Tuberk Toraks 2013; 61(4): 357-359 • doi:10.5578/tt.6268
Geli? Tarihi/Received: 10/09/2013 • Kabul Edili? Tarihi/Accepted: 24/09/2013
Introduction
Postoperative pleural adhesion becomes the clinical problem in some patients with poor respiratory functional impairment. Improper placement of chest tube may cause iatrogenic lung injury. We report herein a case with pneumothorax with complicated pleural adhesion in an elderly, who was successfully evaluated pneumothorax using chest computerized tomography (CT) scan.
Case report
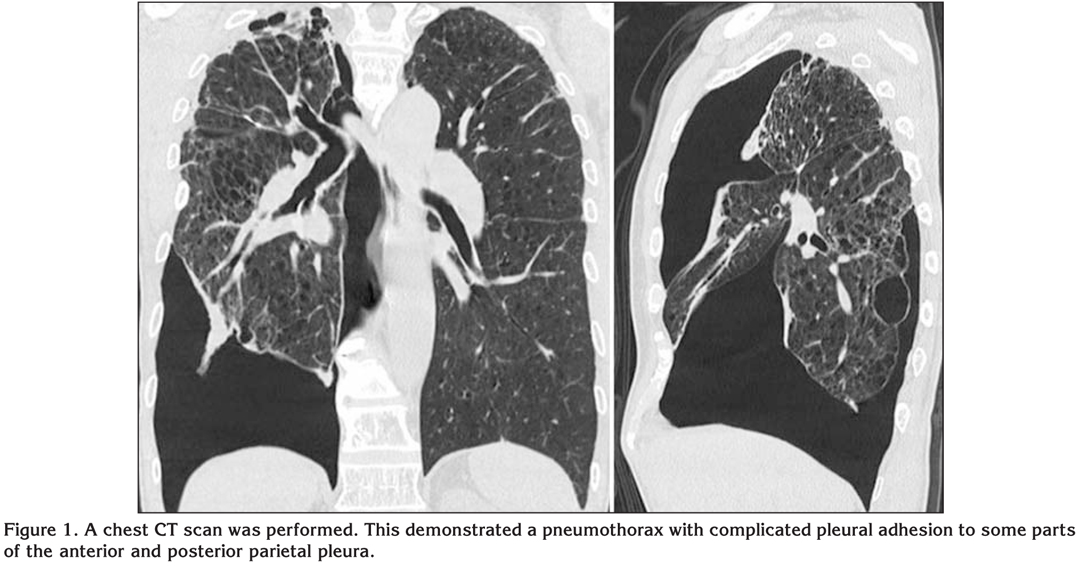
A 77-year-old man presented with acute breathlessness. He had a history of smoking 20 cigarettes per day for 45 years, but stopped smoking at the age of 74. He had pneumothorax of the right three times, which was treated surgically two times. On arrival, he was clear and ambulatory. The vital signs were stable: blood pressure was 130/80 mmHg, pulse rate 84 beats per minute, respiratory rate 16 breaths per minute, and body temperature 37.0?C. Physically, auscultation of the lung revealed clear breath sounds except over the left lung field where breath sounds were diminished. The remainder of the physical examination was unremarkable. A plain chest radiograph demonstrated a right pneumothorax with complicated pleural adhesion. Arterial blood gas analysis revealed that PaO2 was 64.2 torr, PaCO2 43.2 torr, and pH 7.418. As the postero-anterior radiograph demonstrated a pneumothorax with pleural adhesion, therefore, a chest CT scan was performed. This demonstrated a pneumothorax with complicated pleural adhesion to some parts of the anterior and posterior parietal pleura (Figure 1). A drainage tube (Aspiration Kit: 6 Fr) was inserted avoiding the pleural adhesion parts not to injure the lung. The complicated pneumothorax was successfully treated with the chest tube.
Discussion
It is well known that postoperative pleural adhesion may develop in any surgeries for pleural or pulmonary lesions, although video-assisted thoracoscopic surgery lowers the incidence of adhesion to the chest wall (1,2,3). In the majority patients, postoperative pleural adhesion rarely becomes the clinical problem unless additional thoracic surgeries are required. But it may become problem in some patients with poor respiratory functional impairment. Improper placement of chest tube may cause iatrogenic lung injury. Complicated adhesion between pleura and chest wall may cause hemothorax which requires emergency operation (4).
Recurrent pneumothoraces, which require chest tube drainage or surgical approach again, develop especially in patients with chronic obstructive pulmonary disease or those with pulmonary fibrosis (5,6). When a recurrent pneumothorax occurs in these patients, it may become an overlooked because its signs and symptoms often resemble those of the underlying lung disease. In these patients, lungs are vulnerable to such injury, which deteriorates cardiopulmonary condition acutely. Breathlessness and chest pain may be the principal symptoms of pneumothorax. The degree of breathlessness may be often related to the degree of pneumothorax, but chest pain may not necessarily be related to the degree of pleural adhesion. In the present patient, he had breathlessness, but did not complain any chest pain.
If postoperative complicated pleural adhesion exists, the insertion of thoracic drain tube may become difficult. In addition, it is supposed that the frequency of iatrogenic pulmonary injury with the insertion of the drain tube becomes higher. Deneuville evaluated morbidity of percutaneous tube thoracostomy in trauma patients, and reported complication rate of improper placement with iatrogenic injuries to the lung or subclavian vein was 7% in 134 percutaneous tube thoracostomy (7). There were some patients with complicated pleural adhesion, who were properly selected chest drainage tube insertion part (8,9,10). To our knowledge, however, there has been no report about the complication rate in patients with COPD or pulmonary fibrosis.
In our patient, management of the postoperative complicated pneumothorax was greatly enhanced by a CT scan. The CT scan confirmed the diagnosis, demonstrated the site and size of the pneumothorax, identified complicated adhesions between visceral pleura and chest wall, and indicated the optimum site of drainage. The plain chest radiograph did not prove to be sufficient for therapeutic decision-making. Therefore, in patients who develop postoperative recurrent pneumothorax, it is mandatory to perform chest CT scan and evaluate the presence of complicated pleural adhesions. To find the optimal insertion part for chest drainage tube, chest CT scan can provide useful information. The degree of complicated pneumothorax seen on the chest CT scan may be difficult to find the optimum site of drainage.
Conflict of interest
None declared.
REFERENCES
- Nakajima J. Secondary spontaneous pneumothorax. Curr Opin Pulm Med 2010; 16: 376-80.
- Knisely BL, Kuhlman JE. Radiographic and computed tomography (CT) imaging of complex pleural disease. Crit Rev Diagn Imaging 1997; 38: 1-58.
- Tanaka K, Hida Y, Kaga K, Kato H, Iizuka M, Cho Y, et al. Video-assisted thoracoscopic surgery lowers the incidence of adhesion to the chest wall but not to the mediastinal and interlobar pleurae. Surg Laparosc Endosc Percutan Tech 2010; 20: 46-8.
- Endo K, Fukai I, Yuki D, Kawano O, Mizuno K, Tanaka H, et al. Incidence of string-like adhesion between thoracic wall and bullae observed during video-assisted thoracic surgery (VATS) for spontaneous pneumothorax. Kyobu Geka 2012; 65: 855-7.
- Guo Y, Xie C, Rodriguez RM, Light RW. Factors related to recurrence of spontaneous pneumothorax. Respirology 2005; 10: 378-84.
- Panos RJ, Mortenson RL, Niccoli SA, King TE Jr. Clinical deterioration in patients with idiopathic pulmonary fibrosis: causes and assessment. Am J Med 1990; 88: 396-404.
- Deneuville M. Morbidity of percutaneous tube thoracostomy in trauma patients. Eur J Cardiothorac Surg 2002; 22: 673-8.
- Collins JA, Samra GS. Failure of chest X-ray to diagnose pneumothoraces after blunt trauma. Anaesthesia 1988; 53: 74?78.
- Henderson SO, Shoenberger JM. Anterior pneumothorax and a negative chest x-ray in trauma J Emerg Med 2004; 26: 231-3.
- Kikuchi N, Satoh H, Ohtsuka M, Sekizawa K. Anterior pneumothorax. J Emerg Med 2005; 29: 485-6.
Yaz??ma Adresi (Address for Correspondence):
Dr. Hiroaki SATOH,
Tsukuba ?niversitesi Mito T?p Merkezi,
Solunum Hastal?klar? Anabilim Dal?,
Mito, 310-0015, Ibaraki - Japan
e-mail: hirosato@md.tsukuba.ac.jp