CASE REPORT
Doi: 10.5578/tt.10649
Tuberk Toraks 2016;64(3):250-252

Moksifloksasin ilişkili trombositopeni: Olgu sunumu
Mustafa ??RT?K1, Ali Ramazan BENLİ2, Mustafa K?ROĞLU3, Onur YAZICI4, Murat ACAT1, Hasan CASİM4, Erdoğan ?ETİNKAYA1
1 Department of Chest Diseases, Faculty of Medicine, Karabuk University, Karabuk, Turkey
1 Karab?k ?niversitesi Tıp Fak?ltesi, G?ğ?s Hastalıkları Anabilim Dalı, Karab?k, T?rkiye
2 Department of Family Medicine, Faculty of Medicine, Karabuk University, Karabuk, Turkey
2 Karab?k ?niversitesi Tıp Fak?ltesi, Aile Hekimliği Anabilim Dalı, Karab?k, T?rkiye
3 Division of Hematology, Department of internal Medicine, Faculty of Medicine, Karabuk University, Karabuk, Turkey
3 Karab?k ?niversitesi Tıp Fak?ltesi, İ? Hastalıkları Anabilim Dalı, Hematoloji Bilim Dalı, Karab?k, T?rkiye
4 Clinic of Chest Diseases, Karabuk Training and Research Hospital, Karabuk University, Karabuk, Turkey
4 Karab?k ?niversitesi, Karab?k Eğitim ve Araştırma Hastanesi, G?ğ?s Hastalıkları Kliniği, Karab?k, T?rkiye
* This case report was presented as a discussion poster at the 18th Annual Congress of the Turkish Thoracic Association (1-5 April, Belek, Antalya).
?ZET
Moksifloksasin ilişkili trombositopeni: Olgu sunumu
İla? kullanımına bağlı trombositopeniler ?eşitli ila?larla ortaya ?ıkabilir. Bu tablo sıklıkla antibiyotiklere bağlı olarak gelişmektedir. Kinolon grubu antibiyotik kullananlarda trombositopeni bildirilmiştir. Ancak moksifloksasine bağlı trombositopeni olguları nadirdir. Sunulan 60 yaşındaki erkek hastada kronik obstr?ktif akciğer hastalığı (KOAH) mevcuttu ve giderek artan nefes darlığı nedeniyle başvurdu. Hastaneye yatırılan olguda moksifloksasin kullanımının ???nc? g?n?nde başlayan trombositopeni saptandı. Diğer trombositopeni nedenlerinin dışlandığı hastada moksifloksasinin kesilmesinden sonra trombosit d?zeyi normale d?nd?.
Anahtar kelimeler: Kronik obstr?ktif, akciğer hastalığı, kinolonlar, trombositopeni
SUMMARY
Moxifloxacin related thrombocytopenia: A case report*
Drug-induced thrombocytopenia can be caused by various medications, most frequently, antibiotics. There have been reports of thrombocytopenia cases due to the usage of quinolone antibiotics, although moxifloxacin-related thrombocytopenia has been reported very rarely. The case is here presented of a 60-year old male with chronic obstructive pulmonary disease who presented with complaints of progressively worsening dyspnea. After hospitalization, progressive thrombocytopenia was detected which had started on the 3rd day of moxifloxacin treatment. Other causes of thrombocytopenia were excluded and the thrombocyte count returned to normal after discontinuation of moxifloxacin.
Key words: Chronic obstructive, pulmonary disease, quinolones, thrombocytopenia
Geliş Tarihi/Received: 19.09.2015 - Kabul Ediliş Tarihi/Accepted: 13.02.2016
INTRODUCTION
Clinical conditions of drug-related thrombocytopenia (DRT) can vary from immune thrombocytopenia to thrombotic thrombocytopenic purpura (1). DRT most frequently develops from antibiotics, the most common of which are rifampicin, vancomycin, linezolid and sulphonamides (2). Especially in cases where the inpatient has a serious infection or surgery is performed, drug-induced thrombocytopenia may be overlooked.?
Although other quinolone-related thrombocytopenia cases have been reported in literature, there are very few reports of moxifloxacin-related thrombocytopenia (3-5). In this paper, a case of moxifloxacin-related thrombocytopenia is presented and discussed.
CASE REport
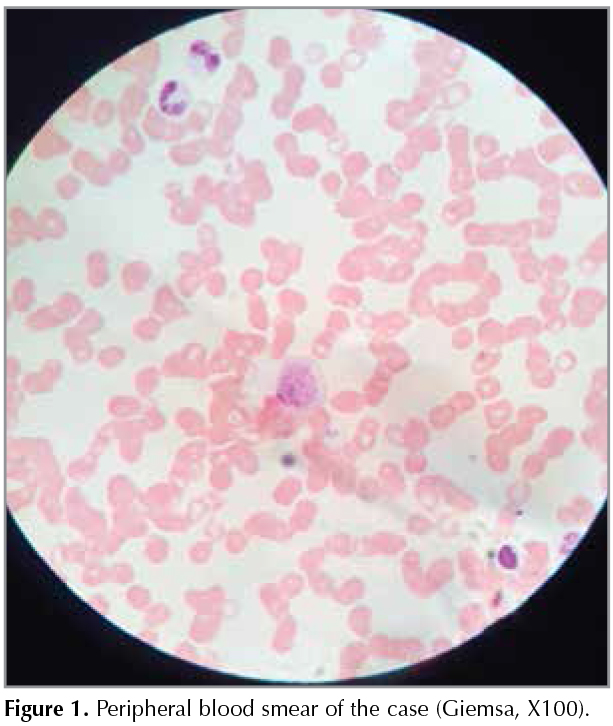
A 60-year old male patient presented at the Emergency Department with worsening dyspnea. The patient had a 5-year history of chronic obstructive pulmonary disease (COPD) and cor pulmonale for 2 years. There was no history of quinolone antibiotic use in previous hospitalization or of thrombocytopenia. It was learned that the patient was not using the bronchodilator medication properly at home.? Arterial blood pressure was 113/68 mmHg, heartrate 98 beats per minute, respiratory rate 26 per minute and oxygen saturation was 89% at room air. On the first day of hospitalization, the hemogram, C-reactive protein (CRP) and biochemical parameters were in the normal range. The systemic examination was normal except for bilateral rhonchus and slight wheezing on respiratory examination. The patient was hospitalized for COPD; nasal oxygen, ipratropium bromide with nebulization, salbutamol and formoterol and intravenous theophylline were administered. It was decided to continue the Diltiazem and furosemide medication which had been prescribed for pulmonary hypertension. There was no alteration on the chest X-Ray which was performed due to increased dyspnea, increased cough and development of purulent sputum on the 3rd day of hospitalization. In the laboratory tests performed as control tests, CRP was 41 mg/L and leukocyte count was 12.300/mm3 (78% granulocyte, +++ toxic granulation) and no other pathology was determined. Considering early onset of hospital-acquired infection, 400 mg/day of intravenous moxifloxacin and 2 g/day intravenous ceftriaxone was administered.? No fever was detected on follow-up. On the 3rd day of antibiotherapy, the CRP value had decreased to 23 mg/L and leukocyte count to 9600/?L, although the thrombocyte count was 72.000/?L. In subsequent daily hemogram controls, the thrombocyte count was 43.000 ?L and 21.000 ?L, respectively. Thrombocytopenia was confirmed with a peripheral blood smear (PBS) (Figure 1). No schistocytes or blast occurrence were detected in the PBS. Acute leukaemia, myelodysplasia and thrombotic thrombocytopenic purpura were excluded. Giant and large thrombocytes which are seen in immune thrombocytopenia were identified in the PBS. Hepatitis markers, coombs test, prothrombin time, active partial thromboplastin time and abdominal ultrasonography were normal. Antinuclear antibody and rheumatoid factor tests were negative. No septic clinical condition was detected and no heparin or low-molecular-weight heparin was administered. Moxifloxacin was discontinued but ceftriaxone was maintained. During the follow-up, the thrombocyte count was > 100.000/?L on the 3rd day. No thrombocytopenia-related hemorrhage developed.
DISCUSSION
Moxifloxacin is an antibiotic of the fluoroquinolone group and is frequently used in the treatment of both outpatients and inpatients. The most common side-effects are nausea, diarrhea, headache and dizziness and less frequently, tendinitis, prolongation of QT gap, aplastic anemia, agranulocytosis and pancytopenia (4). However, isolated thrombocytopenia is rare (3-5). In the current patient, although there were improvements in the infection parameters after the initiation of moxifloxacin therapy, the thrombocytopenia recovered after discontinuing the medication on the consideration of DRT due to the decreased thrombocyte count seen in the laboratory tests.
DRT is classified by the criteria of definite, probable, possible and unlikely (2). The current case was classified as probable according to this classification as moxifloxacin was not used before and was not used again after this clinical condition.
The clinical condition of the thrombocytopenia which emerges may vary from asymptomatic thrombocytopenia to serious hemorrhage. Although the complication of hemorrhage has been reported in 3 previous cases, no hemorrhage was detected in the current case and thrombocyte replacement was not required (3-5).
Generally, thrombocytopenia appears after 1 week of drug administration and returns to normal after 4-8 days of discontinuing the medication (3). In a study by Coker et al. (3), it was reported that the emergence of thrombocytopenia varies between 3-17 days depending on previous fluoroquinolone-related thrombocytopenia. A possible reason for the early detection of thrombocytopenia in this particular case might be that the patient was closely monitored and the drug was administered intravenously.
There should be a high level of suspicion of DRT when there has been drug usage within the previous 5-7 days and there is no other clear cause of thrombocytopenia (2).? However, a differential diagnosis must be applied. In the current case, abdominal ultrasonography for exclusion of hypersplenism, PBS and other laboratory tests for exclusion of diseases such as microangiopathic hemolytic anemia, collagen tissue disease, hepatitis and sepsis were applied. Heparin-related thrombocytopenia was not considered as the patient had not received any heparin. Antiplatelet antibody was not tested as the sensitivity of this test is doubtful (1).
In conclusion, although very rare, thrombocytopenia is a possible side-effect of the use of moxifloxacin. In the differential diagnosis, moxifloxacin-related thrombocytopenia must be considered especially when thrombocytopenia has developed within a few days of starting the medication.
REFERENCES
- Aster RH, Curtis BR, McFarland JG, Bougie DW. Drug-induced immune thrombocytopenia: pathogenesis, diagnosis, and management. J Thromb Haemost 2009;7:911-8.
- Aster RH, Bougie DW. Drug-induced immune thrombocytopenia. N Engl J Med 2007;357:580-7.
- Coker TJ. Drug-induced immune thrombocytopenia due to moxifloxacin. BMJ Case Rep 2013;2013.
- Surana SP, Sardinas Z, Multz AS. Moxifloxacin (avelox) induced thrombotic thrombocytopenic purpura. Case Rep Med 2012;2012:459140.
- Mailman JF, Stigant C, Martinusen D. Moxifloxacin-induced immune-mediated thrombocytopenia in a chronic kidney disease patient receiving hemodialysis. Ann Pharmacother 2014;48:919-22.
Yazışma Adresi (Address for Correspondence)
Dr. Mustafa ??RT?K
Karab?k ?niversitesi Karab?k Eğitim ve Araştırma Hastanesi,
Şirinevler Mah. Alpaslan cad. No:1 Merkez,
KARAB?K - TURKEY
e-mail: mcortuk@yahoo.com