RESEARCH ARTICLE
Doi: 10.5578/tt.27626
Tuberk Toraks 2017;65(1):25-31

Kronik obstr?ktif akciğer hastalığı alevlenme olgularında
başvuru n?trofil lenfosit oranı ile prognoz arasındaki ilişki
Shaghayegh RAHIMIRAD1, Mohammad Reza GHAFFARY1, Mohammad Hossein RAHIMIRAD1, Farid RASHIDI1
1 Department of Respiratory Medicine, Tuberculosis and Lung Research Center, Tabriz University of Medical Sciences,
Tabriz, Iran
1 Tebriz ?niversitesi Tıp Bilimleri, T?berk?loz ve Akciğer Araştırma Merkezi, Solunum Anabilim Dalı, Tebriz, İran
?ZET
Kronik obstr?ktif akciğer hastalığı alevlenme olgularında başvuru n?trofil lenfosit oranı ile prognoz arasındaki ilişki
Giriş: N?trofil lenfosit (NLO), hesaplanmış n?trofil lenfosit (h-NLO), platelet lenfosit (PLO) ve lenfosit monosit (LMO) oranlarının ?eşitli hastalıklarda prognoz tahmininde ?nemli olduğu g?sterilmiştir. Bildiğimiz kadarı ile bu oranların kronik obstr?ktif akciğer hastalığı (KOAH) alevlenmesi olgularında incelendiği ?alışma bulunmamaktadır. Bu ?alışmanın amacı bu parametrelerin KOAH alevlenme nedeni ile hastanede yatan olguların hastane yatış mortalitesini tahminindeki faydasını araştırmaktır.?
Hastalar ve Metod: Bu ?alışma İran'daki Tebriz ve Urmia şehirlerindeki iki hastanede yapılan retrospektif bir ?alışmadır. KOAH alevlenme tanılı olguları başvuru hemogram sonu?larından NLO, PLO, LMO ve h-NLO hesaplandı. Hastanede yatarken ?len ve şifa ile taburcu olan olguların sonu?ları karşılaştırıldı.?
Bulgular: Toplam 315 olgunun 70 (%22.2)'i hastanede ?ld?. Kalan 245 (%77.8) olgu şifa ile taburcu edildi. NLO ≥ 4 olanlarda NLO < 4 olanlara g?re mortalite daha y?ksekti (%24'e karşın %9.5 p< 0.001). Multivariate analizlere g?re NLO (p= 0.001) hastane mortalitesinin bağımsız g?stergelerinden birisiydi.? NLO hem univariate (OR= 3.80) hem multivariate (OR= 3.50) analizlerde en y?ksek odds ratioya (OR) sahipti. NLO i?in eğri altında kalan alan (ROC) 0.72 (%95 CI: 0.62-0.81; p< 0.001) idi. PLO ve LMO ile hastane mortalitesi arasında istatistiksel anlamlı ilişki saptanmadı.
Sonu?: İlk kez bu ?alışmada KOAH alevlenme ile başvuran hastalarda hastane mortalitesi ile NLO arasında istatistiksel anlamlı ilişki olduğu g?sterildi.
Anahtar kelimeler: Kronik obstr?ktif akciğer hastalığı, hastanede yatış mortalitesi, KOAH alevlenme, n?trofil lenfosit oranı, platelet lenfosit oranı
SUMMARY
Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease
Introduction: The prognostic significance of neutrophil-to-lymphocyte ratio (NLR), derived-neutrophil-to-lymphocyte ratio (d-NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) have been shown in many diseases. To the best of our knowledge, there is no published report evaluation of those parameters in acute exacerbation of chronic obstructive pulmonary disease (AECOPD). The aims of this study are to evaluate the parameters in predicting in-hospital mortality in patients with AECOPD.
Materials and Methods: This is a retrospective study in two referral hospitals in Tabriz and Urmia, Iran. NLRs, PLR, LMR, and d-NLR were calculated from the admission day complete blood count of patients with AECOPD. Comparison was made between patients who died in hospital and those discharged alive.
Results: Of 315 patients, 70 (22.2%) died in the hospital and 245 (77.8%) were discharged alive. The mortality rate was higher in patients with NLR ≥ 4 than with NLR < 4 (24% vs. 9.5% p value < 0.001). Multivariate analysis revealed NLR (p= 0.001) were independently associated with in-hospital mortality. NLR had the highest odds ratio for death both in univariate (OR= 3.80) and multivariate (OR= 3.50) analyses. The area under the receiver-operating characteristic curve for NLR in predicting in-hospital death was 0.72 (95% CI: 0.62-0.81; p< 0.001). PLR and LMR did not show significant relation to in-hospital death in AECOPD.
Conclusion: This study shows for the first time that higher NLR is positively associated with in-hospital mortality in AECOPD.
Key words: Chronic obstructive pulmonary disease, hospital mortality, acute exacerbation chronic obstructive pulmonary disease, neutrophil-lymphocyte ratio, platelet-to-lymphocyte ratio
Geliş Tarihi/Received: 21.01.2016 • Kabul Ediliş Tarihi/Accepted: 31.03.2017
INTRODUCTION
The World health organization (WHO) in fact sheet number 315 (March 2015) stated that: "Chronic obstructive pulmonary disease (COPD) is a life-threatening lung disease that interferes with normal breathing. It is more than a "smoker's cough". More than 3 million people died of COPD in 2012, which is equal to 6% of all deaths globally that year. More than 90% of COPD deaths occur in low- and middle-income countries." (1).
COPD was ranked as the sixth cause of death in 1990, will become the third leading cause of death worldwide by 2020. Acute exacerbations of COPD (AECOPD) are the most common causes of hospitalization and death among COPD patients (2). Different biochemical markers have been used in AECOPD patients to predict the outcome; however, many of them are time consuming with extra cost.
It has been well recognized that inflammation plays an important role in COPD. Therefore, circulating biomarkers that reflect the status of inflammation can serve as potential predictors for the prognosis of AECOPD patients.
In recent years, peripheral blood neutrophil-to-lymphocyte ratio (NLR), derived-neutrophil-to-lymphocyte ratio (d-NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) are widely investigated as useful predictors for prognosis in many disease (3).
NLR is a predictor of mortality in several diseases (4). Elevated NLR was an independent prognostic factor for chronic kidney disease, diabetes mellitus, coronary artery disease, appendicitis, systemic lupus erythematosus, Sjogren syndrome, and cystic fibrosis (5-12). In several other diseases, an elevated NLR has been implicated as the marker of a poorer outcome. In patients with stage 4 chronic kidney disease, those with an NLR > 3 had a worse prognosis and a significantly faster progression to the dialysis (5).
However, to the best of our knowledge, only one study in COPD patients, by Gunny et al., showed that in AECOP patients NLR was higher than in stable COPD, and in stable COPD higher than in control. They haven't studied the relation to outcome (13). LMR, d-NLR, and PLR have not been studied in COPD so far.
The aim of this study was to detect a relationship between simple, inexpensive, and easily available NLR, d-NLR-PLR, and LMR parameters with outcome in AECOPD.
MATERIALS and METHODS
This is a retrospective study of patients who were hospitalized with AECOPD in two referral centers in the cities of Tabriz (Imam-Reza hospital) and Urmia (Imam-Khomeini hospital), Iran, from July 2012-2015. Hospital charts were reviewed for admission day CBC parameters (Hematology cell counter Technikon H1, USA). Patients with coexistent hematologic or malignant disorders or those patients with discharge on own consent, were excluded.
Statistical Analysis
We used SPSS 23 IBM software for analysis. We grouped patients with AECOPD to two groups, those who died in hospital and those who discharged hospital alive. We have made comparison of two groups, and p< 0.05 was considered statistically significant. The CBC parameters were entered to SPSS software. Then NLR, PLR, LMR, d-NLR were computed as new variables by SPSS "transform, compute" orders. NLR and PLR were calculated as the ratio of the neutrophils and platelets to lymphocytes, and LMR from lymphocytes to monocytes counts. d-NLR was calculated by dividing the absolute neutrophil count by the difference between leukocytes and neutrophil count [d-NLR= Neutrophil count to (white cell count-neutrophil count)].
Categorical data were described as frequencies and were compared using the chi-square test. To test the normal distribution, we used the Kolmogorov-Smirnov test. Differences in the continuous variables between groups were determined using Student's t-test or the Mann-Whitney U test for variables with or without normal distribution, respectively. Thereafter, we entered variables with significant association with mortality (p< 0.05) in univariate analysis to binary logistic regression analysis, with the "Enter" method. We used receiver-operating characteristic (ROC) curve analysis to identify the best discriminatory cut-off value for NLR, PLR, LMR, and d-NLR.
RESULTS
In total, 315 hospital charts were reviewed, and their demographic characteristics are presented in Table 1. Of 315 patients, 70 (22.2%) patients died in hospital and 245 (77.8%) left hospital alive. Tables 2 and 3 show univariate analysis and comparison of two groups of AECOPD (death in hospital and discharged alive) for categorical and continuous variables, respectively. NLR, d-NLR, anemia, thrombocytopenia, old age, and male sex had statistically significant association with in-hospital mortality. PLR, monocyte count, and presence of comorbidity were not statistically significant (p> 0.05). We used the binary logistic regression model to evaluate the values of age, sex, NLR, anemia, and thrombocytopenia as independent risk factors for in-hospital mortality. NLR showed the highest odds ratio, both in univariate analysis (Table 2, odds= 3.80), and in binary logistic regression analysis (Table 4, odds= 3.58).




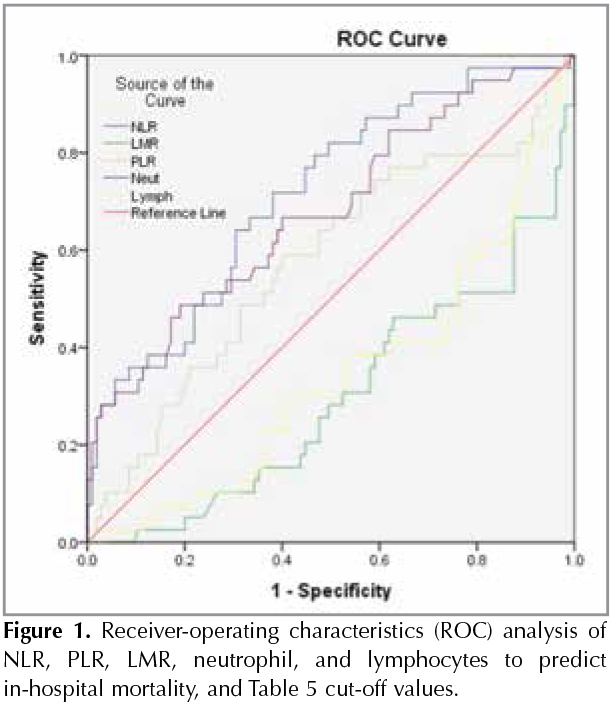
In the ROC curve analysis, the NLR had the highest area under the curve (AUC) value of 0.717 (95% CI, 0.623-0.811) with a cut-off value of 4, and it had a sensitivity of 87%, specificity of 40%. Table 5 and Figure 1 show ROC curve results for NLR, LMR, PLR, neutrophils, and lymphocytes.

DISCUSSION
This study is the first to our knowledge that shows the association of NLR with mortality in patients with AECOPD. NLR was more predictive than neutrophil and lymphocyte counts alone because NLR integrates these two inflammatory markers, indicating opposing clinical outcomes. The suggested mechanisms for association of high NLR with poor outcome in cancers, is that a subpopulation of neutrophils suppresses T-cells activation through the production of reactive oxygen species, nitric oxide, and arginase (14,15). Assessment of the NLR gives information about two different immune pathways concomitantly, and is an indicator of the overall inflammatory status of the body. First, neutrophils that are responsible for lasting inflammation and second, the pathway that is related to lymphocytes, which have a regulatory function (16).
There are no similar studies in AECOPD; however, these findings are consistent with several other studies in other inflammatory diseases. Elevated NLR associated with increased tumor necrosis factor (TNF) alpha, and interleukins of IL-6, IL-7, IL-8, IL-12, and IL-17 (17,18). These markers associated with poor outcome in critically ill patients. In patients with acute-on-chronic liver failure the NLR was an independent predictor for three-month mortality (19). Dirican et al., after studying 116 patients with sarcoidosis, reported that NLR increases with increasing stage of sarcoidosis (20). In a study by Aktimur et al. NLR value (> 9.9) was a diagnostic marker of acute mesenteric ischemia (21). Among the CBC components, only NLR was associated with gangrenous appendicitis (9). It has been suggested that elevated NLR has a better prognostic value than white blood cell count or C-reactive protein in acute appendicitis (22). In patients with acute atrial fibrillation successfully converted to sinus rhythm with amiodarone, those with high NLR had a higher rate of recurrence in the long-term follow up (23). Deng et al. with studying of 389 patients who had undergone gastrectomy, reported that preoperative NLR and d-NLR are prognostic biomarkers in patients with gastric cancer (24). The NLR has been used to predict outcomes in non-alcoholic fatty liver cystic fibrosis (12,25). NLR predicts long-term mortality in patients with ST-segment elevation myocardial infarction (26). A high pretreatment or preoperative NLR has been reported as an independent poor prognostic factor in cancers of lung, gastric breast, and colon (24,27-29). Tropan and co-workers showed in multivariate analysis an independent significant association between high NLR and poor outcome in 290 patients with diffuse large B-cell lymphoma (30).
In our study, there was a relation of mortality with d-NLR. This is expected and may have the same value and mechanism of NLR, there is no rational to calculate D-NLR. Only two studies have showed? prognostic importance of d-NLR in colorectal cancer and gastric cancer (3,24). To the best of our knowledge, there is no study of d-NLR in non-cancer patients.
In our study, there was no association between PLR and mortality rate in the patients with AECOPD. This can be explained by the fact that both numerator (platelet count) and denominator (lymphocyte count) have changed in the similar direction, that is, decrement of both platelet and lymphocyte are associated with increased inpatient mortality rate. To the best of our knowledge, this is the first study of prognostic significance of PLR on the AECOPD patients. Platelets play an important role in inflammation. Thrombocytopenia is associated with poor outcome in AECOPD and several other diseases (31-35). Association of lymphopenia with mortality has already shown in sepsis, in critically ill emergency general surgical patients, and heart failure (36,37).
In our study, anemia also was associated with high mortality in AECOPD. Similar findings are reported in other studies (38).
In univariate analysis, LMR and lymphocyte count, but not monocyte count, showed significant association with mortality rate (p< 0.05); however, in multivariate analysis, LMR showed no association. This discrepancy is due to the higher impact of low lymphocyte count on the calculations, which is not affected significantly by the monocyte count.
Most reported studies about LMR are in malignant diseases, and there are rare studies in non-malignant diseases.? Some studies showed association low LMR with tuberculosis (39,40). It is expected, monocytes are target cells for mycobacterial growth and lymphocytes are the major effectors for mycobacterial clearance (40).
The main limitation of our study is its retrospective nature; however, this limitation may be an advantage of a study that has no bias in management and discharge of patients.
Conclusion
Our results proved our hypothesis and indicated elevated NLR was a respective independent prognostic biomarker for in-hospital mortality in AECOPD. NLR was found to have a superior prognostic value with the highest sensitivity and specificity and the largest AUC, and the highest odds ratio for mortality in AECOPD. However LMR and PLR failed to show prognostic significance. We suggest the NLR, which is cheap and easily measurable even in the simplest health-care units, is practical to use for the follow-up of AECOPD.
REFERENCES
- World Health Organization (WHO). Chronic obstructive pulmonary disease (COPD), Fact sheet,? March 2015.? Accessed date: 2016 Jun 3. Available from: http://www.who.int/mediacentre/factsheets/fs315/en/.
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD, 2016. Accessed date: 2016 Jun 3. Available from: http://goldcopd.org/.
- Ying HQ, Deng QW, He BS, Pan YQ, Wang F, Sun HL, et al. The prognostic value of preoperative NLR, d-NLR, PLR and LMR for predicting clinical outcome in surgical colorectal cancer patients. Med Oncol 2014;31:305.
- Balta S, Demirkol S, Unlu M, Arslan Z, Celik T. Neutrophil to lymphocyte ratio may be predict of mortality in all conditions. Br J Cancer 2013;109:3125-6.
- Kocyigit I, Eroglu E, Unal A, Sipahioglu MH, Tokgoz B, Oymak O, et al. Role of neutrophil/lymphocyte ratio in prediction of disease progression in patients with stage-4 chronic kidney disease. J Nephrol 2013;26:358-65.
- Yilmaz H, Ucan B, Sayki M, Unsal I, Sahin M, Ozbek M, et al. Usefulness of the neutrophil-to-lymphocyte ratio to prediction of type 2 diabetes mellitus in morbid obesity. Diabetes Metab Syndr 2015;9:299-304.
- Poludasu S, Cavusoglu E, Khan W, Marmur JD. Neutrophil to lymphocyte ratio as a predictor of long-term mortality in African Americans undergoing percutaneous coronary intervention. Clin Cardiol 2009;32:E6-E10.
- Kahramanca S, Ozgehan G, Seker D, Gokce EI, Seker G, Tunc G, et al. Neutrophil-to-lymphocyte ratio as a predictor of acute appendicitis. Ulus Travma Acil Cerrahi Derg 2014;20:19-22.
- Ishizuka M, Shimizu T, Kubota K. Neutrophil-to-lymphocyte ratio has a close association with gangrenous appendicitis in patients undergoing appendectomy. Int Surg 2012;97:299-304.
- Li L, Xia Y, Chen C, Cheng P, Peng C. Neutrophil-lymphocyte ratio in systemic lupus erythematosus disease: a retrospective study. Int J Clin Exp Med 2015;8:11026-31.
- Hu ZD, Sun Y, Guo J, Huang YL, Qin BD, Gao Q, et al. Red blood cell distribution width and neutrophil/lymphocyte ratio are positively correlated with disease activity in primary Sjogren's syndrome. Clin Biochem 2014;47:287-90.
- O'Brien CE, Price ET. The blood neutrophil to lymphocyte ratio correlates with clinical status in children with cystic fibrosis: a retrospective study. PLoS One 2013;8:e77420.
- Gunay E, Sarinc Ulasli S, Akar O, Ahsen A, Gunay S, Koyuncu T, et al. Neutrophil-to-lymphocyte ratio in chronic obstructive pulmonary disease: a retrospective study. Inflammation 2014;37:374-80.
- Muller I, Munder M, Kropf P, Hansch GM. Polymorphonuclear neutrophils and T lymphocytes: strange bedfellows or brothers in arms? Trends Immunol 2009;30:522-30.
- Pillay J, Kamp VM, van Hoffen E, Visser T, Tak T, Lammers JW, et al. A subset of neutrophils in human systemic inflammation inhibits T cell responses through Mac-1. J Clin? Invest 2012;122:327-36.
- Celikbilek M, Dogan S, Akyol L, Borekci E, Zararsiz G, Kozan M, et al. Neutrophil-lymphocyte ratio in patients with familial Mediterranean fever. J Clin Lab Anal 2015;29:80-3.
- Motomura T, Shirabe K, Mano Y, Muto J, Toshima T, Umemoto Y, et al. Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J Hepatol 2013;58:58-64.
- Turkmen K, Guney I, Yerlikaya FH, Tonbul HZ. The relationship between neutrophil-to-lymphocyte ratio and inflammation in end-stage renal disease patients. Ren Fail 2012;34:155-9.
- Chen L, Lou Y, Chen Y, Yang J. Prognostic value of the neutrophil-to-lymphocyte ratio in patients with acute-on-chronic liver failure. Int J Clin Pract 2014;68:1034-40.
- Dirican N, Anar C, Kaya S, Bircan HA, Colar HH, Cakir M. The clinical significance of hematologic parameters in patients with sarcoidosis. Clin Respir J 2016;10:32-9.
- Aktimur R, Cetinkunar S, Yildirim K, Aktimur SH, Ugurlucan M, Ozlem N. Neutrophil-to-lymphocyte ratio as a diagnostic biomarker for the diagnosis of acute mesenteric ischemia. Eur J Trauma Emerg Surg 2016;42:363-8.
- Markar SR, Karthikesalingam A, Falzon A, Kan Y. The diagnostic value of neutrophil: lymphocyte ratio in adults with suspected acute appendicitis. Acta Chir Belg? 2010;110:543-7.
- Karavelioglu Y, Karapinar H, Yuksel M, Memic K, Sarak T, Kurt R, et al. Neutrophil to lymphocyte ratio is predictor of atrial fibrillation recurrence after cardioversion with amiodarone. Clin Appl Thromb Hemost 2015;21:5-9.
- Deng Q, He B, Liu X, Yue J, Ying H, Pan Y, et al. Prognostic value of pre-operative inflammatory response biomarkers in gastric cancer patients and the construction of a predictive model. J Transl Med 2015;13:66.
- Alkhouri N, Morris-Stiff G, Campbell C, Lopez R, Tamimi TA, Yerian L, et al. Neutrophil to lymphocyte ratio: a new marker for predicting steatohepatitis and fibrosis in patients with nonalcoholic fatty liver disease. Liver Int 2012;32:297-302.
- Nunez J, Nunez E, Bodi V, Sanchis J, Minana G, Mainar L, et al. Usefulness of the neutrophil to lymphocyte ratio in predicting long-term mortality in ST segment elevation myocardial infarction. Am J Cardiol 2008;101:747-52.
- Kang MH, Go SI, Song HN, Lee A, Kim SH, Kang JH, et al. The prognostic impact of the neutrophil-to-lymphocyte ratio in patients with small-cell lung cancer. Br J Cancer 2014;111:452-60.
- Azab B, Bhatt VR, Phookan J, Murukutla S, Kohn N, Terjanian T, et al. Usefulness of the neutrophil-to-lymphocyte ratio in predicting short- and long-term mortality in breast cancer patients. Ann Surg Oncol 2012;19:217-24.
- Chang Z, Zheng J, Ma Y, Zhao J, Wang C, Liu Z. The neutrophil-to-lymphocyte ratio as a predictor for recurrence of colorectal liver metastases following radiofrequency ablation. Med Oncol 2014;31:855.
- Troppan K, Deutsch A, Gerger A, Stojakovic T, Beham-Schmid C, Wenzl K, et al. The derived neutrophil to lymphocyte ratio is an independent prognostic factor in patients with diffuse large B-cell lymphoma. Br J Cancer? 2014;110:369-74.
- Rahimi-Rad MH, Soltani S, Rabieepour M, Rahimirad S. Thrombocytopenia as a marker of outcome in patients with acute exacerbation of chronic obstructive pulmonary disease. Pneumonol Alergol Pol 2015;83:348-51.
- Agrawal S, Sachdev A, Gupta D, Chugh K. Platelet counts and outcome in the pediatric intensive care unit. Indian J Crit Care Med 2008;12:102-8.
- Brogly N, Devos P, Boussekey N, Georges H, Chiche A, Leroy O. Impact of thrombocytopenia on outcome of patients admitted to ICU for severe community-acquired pneumonia. J Infect 2007;55:136-40.
- Lopez-Delgado JC, Rovira A, Esteve F, Rico N, Manez Mendiluce R, Ballus Noguera J, et al. Thrombocytopenia as a mortality risk factor in acute respiratory failure in H1N1 influenza. Swiss Med Wkly 2013;143:w13788.
- Moreau D, Timsit JF, Vesin A, Garrouste-Orgeas M, de Lassence A, Zahar JR, et al. Platelet count decline: an early prognostic marker in critically ill patients with prolonged ICU stays. Chest 2007;131:1735-41.
- Drewry AM, Samra N, Skrupky LP, Fuller BM, Compton SM, Hotchkiss RS. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock 2014;42:383-91.
- Vulliamy PE, Perkins ZB, Brohi K, Manson J. Persistent lymphopenia is an independent predictor of mortality in critically ill emergency general surgical patients. Eur J Trauma Emerg Surg 2015.
- Sarkar M, Rajta PN, Khatana J. Anemia in Chronic obstructive pulmonary disease: Prevalence, pathogenesis, and potential impact. Lung India 2015;32:142-51.
- Wang J, Yin Y, Wang X, Pei H, Kuai S, Gu L, et al. Ratio of monocytes to lymphocytes in peripheral blood in patients diagnosed with active tuberculosis. Braz J Infect Dis 2015;19:125-31.
- Naranbhai V, Kim S, Fletcher H, Cotton MF, Violari A, Mitchell C, et al. The association between the ratio of monocytes:lymphocytes at age 3 months and risk of tuberculosis (TB) in the first two years of life. BMC Med? 2014;12:120.
- World Health Organization. Nutritional anaemias: Report of a WHO scientific group. Geneva, Switzerland: 1968.
Yazışma Adresi (Address for Correspondence)
Dr. Mohammad Hossein RAHIMIRAD
Bronchoscopy Unite,
Imam Reza Hospital,
TABRIZ - IRAN
e-mail: rahimirad@hotmail.com