RESEARCH ARTICLE
Tuberk Toraks 2019;67(1):8-14
Plevral plaklarin F-18 FDG PET/CT ve CT ile degerlendirilmesi
Zehra Pınar KO?1, Pelin ?ZCAN KARA1, Y?ksel BALCI2, G?lhan ?REKİCİ3, Rabia BOZDOĞAN ARPACI4, Eylem SERCAN ?ZG?R5
1 Mersin ?niversitesi Tıp Fak?ltesi, N?kleer Tıp Anabilim Dalı, Mersin, T?rkiye
1 Department of Nuclear Medicine, Faculty of Medicine, Mersin University, Mersin, Turkey
2 Mersin ?niversitesi Tıp Fak?ltesi, Radyoloji Anabilim Dalı, Mersin, T?rkiye
2 Department of Radiological, Faculty of Medicine, Mersin University, Mersin, Turkey
3 Mersin ?niversitesi Tıp Fak?ltesi, Biyoistatistik Anabilim Dalı, Mersin, T?rkiye
3 Department of Biostatistics, Faculty of Medicine, Mersin University, Mersin, Turkey
4 Mersin ?niversitesi Tıp Fak?ltesi, Patoloji Anabilim Dalı, Mersin, T?rkiye
4 Department of Pathology, Faculty of Medicine, Mersin University, Mersin, Turkey
5 Mersin ?niversitesi Tıp Fak?ltesi Hastanesi, G?ğ?s Hastalıkları Anabilim Dalı, Mersin, T?rkiye
5 Department of Chest Diseases, Faculty of Medicine, Mersin University, Mersin, Turkey
?ZET
Plevral plakların F-18 Fdg Pet/ct ve Ct ile değerlendirilmesi
Giriş: Plevral plakların malign olma olasılığı vardır ve bu antitenin araştırılması ?ok ?nemli olup en ?nemli radyolojik belirte? genel olarak florodeoksiglukoz (FDG) tutulumudur. Ancak bu konu ile ilgili daha ?nceki ?alışmalar ve literat?r bilgileri arasında uyumsuzluklar vardır. Bu ?alışmanın amacı plevral plaklarda standardize tutulum değeri (SUD) ve malignite a?ısından kesim değerinin analizi ve bulguların bilgisayarlı tomografi (BT) ile karşılaştırılmasıdır.
Materyal ve Metod: Yetmiş bir hasta (27 K, 44 E; ortalama yaş: 59.9 ? 13.1) ?alışmaya dahil edilmiştir. Onkolojik ama?lı F-18 FDG PET/BT t?m hastalara uygulanmıştır. Pozitron emisyon tomografi/bilgisayarlı tomografi (PET/BT) g?r?nt?lerinin BT kısmından elde edilen g?r?nt?lerde tanımlanan plevral plaklar bağımsız bir Radyoloji Uzmanı tarafından kontrastlı veya kontrastsız BT g?r?nt?leri ?zerinden değerlendirilmiş ve sonu?lar altın standard patoloji olmak ?zere karşılaştırılmıştır.
Bulgular: Tanısal sensitivite, spesifisite BT i?in %39, %79 sırasıyla ve SUVmax i?in kesim değeri 4.8 kabul edildiğinde PET i?in %71 ve %63 sırasıyla bulunmuştur.
Sonu?: Bizim ?alışmamızın sonu?larına g?re ROC eğrileri ile belirlenen plevral plaklar i?in malignite i?in en uygun kesim değeri 4.8 olarak hesaplanmıştır. Bu kesim değeri kabul edildiğinde PET/BT?nin sensitivite ve doğruluğu BT?ye g?re y?ksek bulunmuştur.?
Anahtar kelimeler: Plevral plaklar, FDG, PET, CT
SUMMARY
The F-18 Fdg Pet/ct and Ct evaluation of pleural plaques
Introduction: Pleural plaques have the possibility of bearing malignancy thus investigation of this entity is important and the most important indicator of malignancy in general is fluorodeoxyglucose (FDG) accumulation in radiological appearance. However there is discrepancy between results of previous studies in the literature about this subject. The aim of this study is to analyze the standardized uptake value of pleural plaques and the cut off levels for malignancy in comparison with computed tomography (CT).
Materials and Methods: Seventy one patients were included in the study (27F, 44M; mean: 59.9 ? 13.1 years). Oncologic F-18 FDG positron emission tomography/computed tomography (PET/CT) was performed to all the subjects for a different primary tumor. Pleural plaques were identified in all patients in CT component of PET/CT examination. Contrast enhanced and nonenhanced CT images were evaluated by a Radiology Physician independently according to the gold standard pathology.
Results: The diagnostic sensitivity, specificity of CT was; 39%, 79% respectively and if the cut-off SUVmax level was accepted "4.8" the diagnostic sensitivity and specificity of PET was 71%, and 63% respectively.
Conclusion: According to the results and ROC curves determined in the study the cut-off level for evaluation of pleural plaques in PET examination was "4.8". The sensitivity and accuracy of PET was higher compared to CT with this cut-off value.
Key words: Pleural plaques, FDG, PET, CT
Geliş Tarihi/Received: 24.09.2018 - Kabul Ediliş Tarihi/Accepted: 06.02.2019
INTRODUCTION
Pleural plaques are one of the manifestations of asbestosis related pleural disease. In the end of this spectrum the patients may develop malignant mesothelioma; a rare and highly mortal malignancy. The first line imaging modality is computed tomography (CT) which can determine the extent of disease (invasion to adjacent structures; mediastinal or dyafragmatic) and accompanying parenchyma or nodal involvement. However CT or magnetic resonance (MR) imaging cannot differentiate malignant and benign pleural plaques sufficiently (1).
F-18 fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET/CT) is a discriminative imaging modality in various types of malignant tumors. It has been investigated whether PET/CT can differentiate malignant and benign pleural disease previously and the diagnostic accuracy of this modality is documented in staging of malignant mesothelioma (2). However the FDG uptake of the pleural plaques was not considered an important determinant previously and there is no documented and/or accepted cut-off value already for malignant/benign plaque discrimination (3).
The aim of this study is to evaluate the discriminative role of FDG uptake in pleural plaques and to determine a cut-off level for malignant plaques in comparison with CT.
MATERIALS and METHODS
Patients
The study was approved by the Institutional Research Ethics Committee. Seventy one patients were subject of this study (27F, 44M; mean: 59.9 ? 13.1 years). The patients were referred to PET/CT examination due to different kinds of malignant tumors or suspicious malignant findings (cancer of primary unknown, solitary pulmonary nodule or pleural malignancy) (Table 1). The patients were informed about the examination and informed consents were obtained. The study was conducted according to the Helsinki Declaration revised in 2010.

FDG PET/CT Imaging
The patients were subjected to the F-18 FDG PET/CT necessarily due to an underlying malignancy (staging, restaging, and treatment response evaluation) or suspicion of a malignant disease. Approximately 10 mCi (370 mBq) F-18 FDG administrations via venous line with saline flush was performed after fasting for at least 4 hours. PET/CT imaging was performed by an integrated PET/CT scanner (GE Discovery PET/CT, 610, USA) by a two step procedure. Firstly a whole body CT scan without intravenous contrast administration with 130 kV, 50 mAs, a pitch of 1.5, a section thickness of 5 mm, and a field of view of 70 cm and just after the CT scan whole body PET imaging was performed with an acquisition time of 3 min per bed position in a three dimensional acquisition mode. In case of solitary pulmonary nodule evaluation late phase (approximately in 2nd hour) images including thorax were provided.
Image Analysis
The PET/CT images were evaluated by two experienced Nuclear Medicine physicians from axial, sagittal and coronal images with additional CT and fusion images. Additionally SUVmax levels of the lesions were determined by the workstation of GE. CT images obtained from the PET/CT scanner was analyzed by an experienced Radiology physician regarding the structure of the lesion (peripheral mass like or not) in an independent manner.
The results of PET/CT and CT were compared according to the gold standard pathology.
Statistical Analysis
The statistical analysis of the variables was performed by MedCalc v10.3.0 program. SUVmax cut-off levels was determined to identify malignancy by receiver operating curve (ROC) analysis and sensitivity and specificity of the tests according to this cut-off level was decided with 95% CI.
RESULTS
Among the 71 patients 21 were out of follow; 3 of them died during the follow up. Fifty patients with histopathological results were evaluated. The PET, BT and histopathological findings are summarized in Table 2.

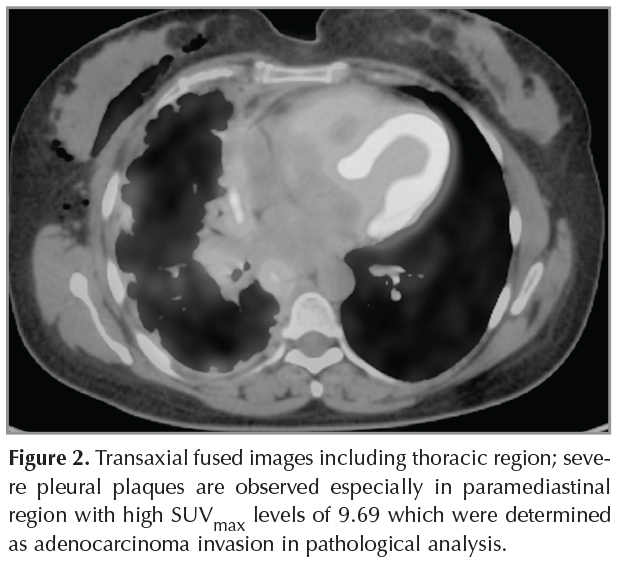
Nine patients? pathology results were malignant mesothelioma two of which was determined by cytology and others by blind needle or thoracoscopic biopsy. Among the patients with malignant mesothelioma diagnosis only two patients had low SUVmax levels (Figure 1). Fifteen patients had benign results (including tuberculosis, granulamatous inflammation, empiyema, pneumonia, pleuritis). One of two patients with neuroendocrine tumors had negative PET estimation. All the remaining patients confirmed pleural invasion of another malignancy or another primary tumor (Figure 2).

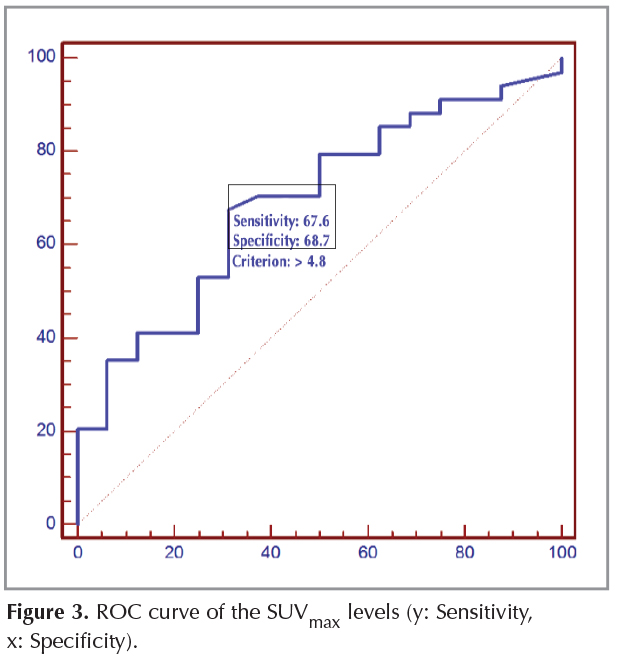
The diagnostic sensitivity, specificity of CT was; 39%, 79% respectively and if the cut-off SUVmax level was accepted ?4.8? the diagnostic sensitivity and specificity of PET was 71%, and 63% respectively (Figure 3).
The diagnostic sensitivity, specificity, accuracy, PPV and NPV of CT and PET (according to 4.8 cut-off value) are summarized in Table 3.

The mean SUVmax levels of the lesions with benign and malignant pathological results were significantly different (n= 15; 5.1 ? 2.7 and n= 35; 7.1 ? 4.3 (p= 0.054) respectively) (Figure 4).

DISCUSSION
Pleural plaques need a challenging workout in order to make accurate discrimination between malignant and benign lesions. It is important to determine a cut-off value but also difficult. Since some of the malignant mesothelioma lesions may not have sufficient FDG uptake and some of the benign lesions might have significant FDG uptake and significant overlap exists between SUVmax levels of benign and malignant lesions. However according to our results the mean SUVmax levels of the benign and malignant lesions are significantly different. Additionally this study has opportunity to have pathological confirmation of pleural lesions. In this study it was not possible to provide high sensitivity or specificity levels for neither PET/CT nor CT. However it was possible to determine a cut-off level for pleural lesions to discriminate malignant and benign lesions which was ?4.8?.
Kurata et al. have investigated the role of PET and osteopontin levels in asbestos related pleural disease and concluded that malignant mesothelioma has significantly higher uptake than benign asbestos related pleural disease (1). There is limited number of studies in the literature about asbestos related pleural disease in the literature (3). Kurata et al. accepted a SUVmax level of 4.1 and Orki et al. as 3.0 for determination of malignancy (1,3). However the authors stressed about the epitheloid subtype of malignant mesothelioma which is a slow growing variant of the group that has SUVmax levels around 2.0 (1). In this study there were two patients with similar uptake values who were decided to have malignant mesothelioma.
Unfortunately the number of patients with malignant pleural disease is increasing in recent years because of the workers who are exposed to the asbestos related products (4). Additionally there are specific regions in which their soils include asbestos and people built their houses with this material as in our country. These reasons may be related to the relative higher SUVmax levels in our study.
Diffuse pleural disease consists of the diffuse involvement of visceral pleura rather than parietal pleura; with significant definition on CT scan (4,5). In this study the mass like lesion in CT component of PET/CT; which was a non contrast and low dose CT study; was accepted as positive for malignancy in pleural plaques however the diagnostic accuracy of CT alone was not sufficient. Comparative studies with contrast enhanced normal dose CT imaging may be planned in the future.? MR has higher sensitivity and specificity in the discrimination of benign and malignant pleural disease; 98-100% and 92-93% respectively (6). In a recent study comparing the results of FDG PET/CT and dynamic contrast enhanced MRI? in the evaluation of malignant pleural mesothelioma have showed that prognostic information regarding overall survival might be predicted by SUVmax levels while MRI washout curve shape is related with overall survival as well (7). Another prospective study with the patients with diagnosis of unresectable malignant pleural mesothelioma showed that SUVmax is correlated with progression free and overall survival and chemoterahy response potential (8). The results of the study about the response evaluation of pleural mesothelioma to chemotherapy treatment have demonstrated that SUVmax might point out the responders (9).
Previous reports have shown a diagnostic sensitivity of 60-100%, specificity of 78-100% and accuracy of 91-98% (10,11). In a previous study in case of SUVmax level of 2.0 accepted as a cut-off level the sensitivity of FDG PET was 91% and specificity was 100% (12). However the SUVmax cut-off level of 2.5 was significantly not specific in this study. This difference may be consequences of significant number of false positive cases in our country due to benign diseases contribute to high SUVmax levels especially granulamatous diseases like Tuberculosis. Thus it is difficult to determine a certain cut-off level for SUVmax in especially countries with high number of false positive cases. However in case of presence of malignant mesothelioma it is possible to accurately stage the disease especially by showing extrathoracic involvement and provide prognostic information (13,14). Additionally in a previous study in patients with mesothelioma it has been suggested that FDG uptake in pretreatment scan was a significant predictor of survival (15).
The pleural effusion may be observed in most of the patients with mesothelioma in the disease course and may be important to discriminate malignant from benign pleural disease (16,17). In one of two patients with low uptake malignant mesothelioma in this study there was additional pleural effusion as well. In case of additional pleural effusion adjacent to the suspicious pleural lesion the careful interpretation may be necessary regardless of the uptake of the lesion.? Additionally miliary diffuse disease have been reported as case reports in the literature in mesothelioma and lymphangitic disease distribution may be observed in advanced stages of the disease (17-19).
There is limited number of studies investigating the benign and malignant plaque discrimination capacity of FDG PET/CT (16). Elboga et al. investigated the malignancy potential of pleural plaques and found that PET is useful modality in discrimination of malignant and benign plaques and delayed imaging may determine benign disease by showing decreased uptake in late phase (20). There are some large series with significant number of patients in past however those studies include PET only estimation however it is important to determine recent PET/CT scanners? results. As an example talc pleurodesis is another important reason of false positive FDG uptake in pleural plaques that can be discriminated by means of correlation with CT appearance (21,22). Additionally this study has superiority of having CT scan comparison with estimation of a different observer and advantage of the same time study for PET/CT and CT.
Another important finding of this study is the high ratio of malignant disease involvement of pleura. This may be a consequence of the population involved (including patients with different primary tumors) rather than patients who have only suspicious pleural plaques.
Limitations of this study are its retrospective structure and lack of intravenous contrast administered diagnostic CT scan results.
PET/CT might have high enough diagnostic accuracy in comparison with CT in discrimination of benign and malignant pleural plaques with careful evaluation regarding false positive causes and SUVmax cut-off level of ?4.8?.
CONFLICT of INTEREST
The authors reported no conflict of interest related to this article.
AUTHORSHIP CONTRIBUTIONS
Concept/Design: ZPK, P?K, YB
Analysis/Interpretation: All of authors.
Data Acquisition: All of authors.
Writting: ZPK, P?K
Critical Revision: ZPK, P?K
Final Approval: All of authors.
REFERENCES
- Kurata S, Ishibashi M, Azuma K, Takamori S, Fujimoto K, Kobayashi M. Preliminary study of positron emission tomography/computed tomography and plasma osteopontin levels in patients with asbestosos-related pleural disease. Jpn J Radiol 2010;28:446-52.
- Flores RM, Akhurst T, Gonen M, Larson SM, Rusch VW. Positron emission tomography defines metastatic disease but not locoregional disease in patients with malignantant pleural mesothelioma. J Thorac Cardiovasc Surg 2003;126:11-6.
- Orki A, Akin O, Tasci AE, Ciftci H, Urek S, Falay O, et al. The role of positron emission tomography/computed tomography in the diagnosis of pleural diseases. Thorac Cardiovasc Surg 2009;57:217-21.
- Miles SE, Sandrini A, Johnson AR, Yates DH. Clinical consequences of asbestosos-related diffuse pleural thickening: A review. J Occup Med Toxicol 2008;3:20.
- Tiitola M, Kivisaari L, Zitting A, Huuskonen MS, Kaleva S, Tossavainen A, et al. Computed tomography of asbestosos-related pleural abnormalities. Int Arch Occup Environ Health 2002;75:224-8.
- Luo L, Hierholzer J, Bittner RC, Chen J, Huang L. Magnetic resonance imaging in distinguishing malignantant from benign pleural disease. Chin Med J 2001;114:645-9.
- Hall DO, Hooper CE, Searle J, Darby M, White P, Harvey JE, et al. 18F-Fluorodeoxyglucose PET/CT and dynamic contrast-enhanced MRI as imaging biomarkers in malignant pleural mesothelioma. Nucl Med Commun 2018;39:161-70.
- Zucali PA, Lopci E, Ceresoli GL, Giordano L, Perrino M, Ciocia G, et al. Prognostic and predictive role of [18F] fluorodeoxyglucose positron emission tomography (FDG-PET) in patients with unresectable malignant pleural mesothelioma (MPM) treated with up-front pemetrexed-based chemotherapy. Cancer Med 2017;6:2287-96.
- Niccoli Asabella A, Di Palo A, Altini C, Fanelli M, Ferrari C, Lavelli V, et al. 18F-FDG PET/CT in therapy response and in predicting responders or non-responders in malignant pleural mesothelioma patients, by using semi-quantitative mRECIST and EORTC criteria. Hell J Nucl Med 2018;21:191-7.
- Kitajima K, Doi H, Kuribayashi K. Present and future roles of FDG-PET/CT imaging in the management of malignant pleural mesothelioma. Jpn J Radiol 2016;34:537-4.
- Terada T, Tabata C, Tabata R, Okuwa H, Kanemura S, Shibata E, et al. Clinical utility of 18-fluorodeoxyglucose positron emission tomography/computed tomography in malignant pleural mesothelioma. Exp Ther Med 2012;4:197-200.
- B?nard F, Sterman D, Smith RJ, Kaiser LR, Albelda SM, Alavi A. Metabolic imaging of malignantant pleural mesothelioma with fluorodeoxyglucose positron emission tomography. Chest 1998;114:713-22.
- Erasmus JJ, Truong MT, Smythe WR, Munden RF, Marom EM, Rice DC, et al. Integrated computed tomography-positron emission tomography in patients with potentially resectable malignantant pleural mesothelioma: Staging implications. J Thorac Cardiovasc Surg 2005;129:1364-70.
- Flores RM, Akhurst T, Gonen M, Zakowski M, Dycoco J, Larson SM, et al. Positron emission tomography predicts survival in malignantant pleural mesothelioma. J Thorac Cardiovasc Surg 2006;132:763-8.
- Benard F, Sterman D, Smith RJ, Kaiser LR, Albelda SM, Alavi A. Metabolic imaging of malignantant pleural mesothelioma with fluorodeoxyglucose positron emission tomography. Chest 1998;114:713-22.
- Garg K, Lynch DA. Imaging of thoracic occupational and environmental malignantancies. J Thorac Imaging 2002;17:198-210.
- Gevenois PA, de Maertelaer V, Madani A, Winant C, Sergent G, De Vuyst P. Asbestososis, pleural plaques and diffuse pleural thickening: three distinct benign responses to asbestosos exposure. Eur Respir J 1998;11:1021-7.
- Rosenstock L, Hudson, LD. The pleural manifestations of asbestosos exposure. Occup Med 1987;2:383-407.
- Leung AN, M?ller NL, Miller RR. CT in differential diagnosis of diffuse pleural disease. AJR Am J Roentgenol 1990;154:487-92.
- Elboga U, Yılmaz M, Uyar M, Zeki ?elen Y, Bakır K, Dikensoy O. The role of FDG PET-CT in differential diagnosis of pleural pathologies. Rev Esp Med Nucl Imagen Mol 2012;31:187-91.
- Tenconi S, Luzzi L, Paladini P, Voltolini L, Gallazzi MS, Granato F, et al. Pleural granuloma mimicking malignancy 42 years after slurry talc injection for primary spontaneous pneumothorax. Eur Surg Res 2010;44:201-3.
- Kwek BH, Aquino SL, Fischman AJ. Fluorodeoxyglucose positron emission tomography and CT after talc pleurodesis. Chest 200;125:2356-60.
Yazışma Adresi (Address for Correspondence)
Dr. Zehra Pınar KO?
Mersin ?niversitesi Tıp Fak?ltesi,
N?kleer Tıp Anabilim Dalı
Mersin - T?RKİYE
e-mail: zehrapinarkoc@gmail.com